Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]

Heyde’s syndrome is a syndrome of gastrointestinal bleeding from angiodysplasia in the presence of aortic stenosis. Iron deficiency anaemia and aortic stenosis are common in the elderly, but their association with angiodysplasia and bleeding is not generally recognised.
Heyde’s syndrome is a syndrome of gastrointestinal bleeding from angiodysplasia in the presence of aortic stenosis. It is named after Edward C. Heyde, who first noted the association in 1958.1 It is caused by the induction of Von Willebrand disease type IIA (vWD-2A) by a depletion of Von Willebrand factor (vWF) in blood flowing through the narrowed valvular stenosis.2
[rml_read_more]
This case study describes a older, frail woman who presented following a fall resulting in a fragility osteoporotic fracture of the right neck of femur. Following assessment she was found to have severe aortic stenosis and iron deficiency anaemia.
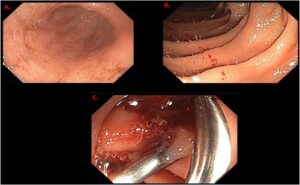
She was managed with blood transfusion, aortic valve replacement by TAVI (trans aortic valvular implantation) and hemiarthroplasty. She also underwent capsular endoscopy following her rehabilitation, which confirmed extensive colonic angiodysplasia as the possible source of the iron deficiency anaemia.
A 75-year-old woman was admitted following a fall witnessed by her son. She did not lose consciousness, but immediately complained of severe pain from the right hip and was unable to stand. Her son mentioned that she had been unwell for the past month with extreme lethargy, fatigue and tiredness.
The patient was diagnosed with Alzheimer’s dementia two years previously. She also had hypertension, osteoarthritis and bilateral cataracts. She was recently investigated for weight loss and iron deficiency anaemia and underwent endoscopy, which was reported as normal.
Further questioning of her carer revealed that she had mild intermittent epistaxis, but no other bleeding areas or change in her bowel habits. The son also mentioned that there is no family history of bleeding tendencies or blood clots.
She is mobile with a Zimmer frame and has a formal carer three times a day. Her clinical frailty scale (Rookwood scale) was 6.
Assessment in A&E revealed a frail lady with pallor. Her abbreviated mental test score was 3 out of 10. Examination of her cardiovascular system showed an ejection systolic murmur in the aortic area radiating to the carotids with soft second heart sound. Pelvis X-ray showed a right subcapital fractured neck of femur.
ECG sinus tachycardia with heart rate of 126 with T waves inversion in lead 1, avl, v5 & v6.
Troponin I levels are within normal limits. Blood tests showed haemoglobin (Hb) levels at 51 (was 102 two month ago), mean corpuscular volume (MCV) 71, white blood cell count (WCC) 7.4, platelets 254, partial thromboplastin time (PTT) 32, international normalised ratio (INR) 1.0, adjusted Ca 2.10 alkaline phosphatase (ALP) 189, Vitamin D 14, with normal U&Es.
Iron studies, coagulation profile and echocardiographic results are shown in box 1.
A working diagnosis of iron deficiency anaemia, aortic stenosis, fall and fractured neck of femur was made. Three units of pack red blood cells were arranged for transfusion.
The patient had another fall while in the ward, but her ECG showed no new changes and her CT brain had no new acute intracranial pathologies. An echocardiography was arranged which showed a severe aortic stenosis with a mean transvalvular gradient of 68.8mmhg, a peak systolic gradient of 136mmhg and valvular flow of 0.7m/s. (Box 1)
The patient was assessed by the cardiology team, who arranged for CT angiography prior to TAVI. The result of the CT angiography showed normal vascular territories. Although current trust guidelines for integrated fracture neck femur state that hemiarthroplasty should be done within 36 hours of admission, it was agreed that the valvular replacement and stabilisation of the patient was a priority. Also as shown in the literature the valvular replacement would reduce the episodes of the gastrointestinal tract (GIT) bleeding
Reviewing her endoscopy results in the clinical web portal did not show specific lesions responsible for the iron deficiency anaemia. This was discussed with the gastroenterology team along with the possibility of angiodysplasia and the need for colonoscopy or capsular endoscopy, which was done after the rehabilitation (Figure 1).
It was also discussed with the haematology team about the possibility of Heyde’s syndrome and whether the patient might need a vWD-2A estimation to complete the triad of the syndrome (GIT bleeding, aortic stenosis, coagulopathy with angiodysplasia). Even though in this patient the repeated blood transfusion may have affected the sensitivity of the results.
Heyde’s syndrome is now known to be gastrointestinal bleeding from angiodysplasia lesions due to acquired vWD-2A deficiency secondary to aortic stenosis, and the diagnosis is made by confirming the presence of those three things.1
Von Willebrand factor is synthesised in the walls of the blood vessels and circulates freely in the blood in a folded form. When it encounters damage to the wall of a blood vessel, particularly in situations of high velocity blood flow, it binds to the collagen beneath the damaged endothelium and uncoils into its active form. Platelets are attracted to this activated form of von Willebrand factor and they accumulate and block the damaged area, preventing bleeding.3
Gastrointestinal bleeding may present as bloody vomit, dark, tarry stool from metabolised blood, or fresh blood in the stool. In a person presenting with these symptoms, endoscopy, gastroscopy, and/or colonoscopy should be performed to confirm the presence of angiodysplasia.3
Angiodysplasia may occur anywhere in the gastrointestinal tract, but is most common in the ascending colon, particularly the caecum. In a prospective study of colonoscopies of 1,938 patients, typical angiodysplasia was found in 3% of cases, but 80% were asymptomatic. The sites of highest prevalence of the lesions were the caecum (37%) and sigmoid colon (18%)
A total of 1–6% of in-patient gastrointestinal bleeds are caused by angiodysplasia, while 30–40% of gastrointestinal bleeds of an obscure source are found to be linked to angiodysplasia and it is possibly the most common cause of lower gastrointestinal bleeding in the elderly. Angiodysplasia are found incidentally in 3% of non-bleeding patients over age of 65 years. They are present in 2.6–6.2% of patients being investigated for gastrointestinal bleeding.4
Aortic stenosis can be diagnosed by auscultation for characteristic heart sounds, particularly a crescendo-decrescendo (i.e., ‘ejection’) murmur, followed by echocardiography to measure aortic valve area. While Heyde’s syndrome may exist alone with no other symptoms of aortic stenosis,2 the person could also present with evidence of heart failure, fainting, or chest pain.5
Finally, Heyde’s syndrome can be confirmed using blood tests for vWD-2A, although traditional blood tests for von Willebrand factor may result in false negatives due to the subtlety of the abnormality. The gold standard for diagnosis is gel electrophoresis; in people with vWD-2A, the large molecular weight von Willebrand factors will be absent from the SDS-agarose electrophoresis plate.2
The definitive treatment for Heyde’s syndrome is surgical replacement of the aortic valve. Recently, it has been proposed that TAVI can also be used for definitive management. Direct surgical treatment of the bleeding (e.g. surgical resection of the bleeding portion of the bowel) is only rarely effective.5
Medical management of symptoms is possible also, although by necessity temporary, as definitive surgical management is required to bring levels of von Willebrand factor back to normal.4 In severe bleeding, blood transfusions and IV fluid infusions can be used to maintain blood pressure.
In addition, desmopressin (DDAVP) is known to be effective in people with von Willebrand’s disease, including people with valvular heart disease. Desmopressin stimulates release of von Willebrand factor from blood vessel endothelial cells by acting on the V2 receptor, which leads to decreased breakdown of Factor VIII. Desmopressin is thus sometimes used directly to treat mild to moderate acquired von Willebrand’s disease and is an effective prophylactic agent for the reduction of bleeding during heart valve replacement surgery.4
Iron deficiency anaemia and aortic stenosis are common in older patients, but their association with angiodysplasia and bleeding is not generally recognised. Heyde syndrome is a complex disorder, resulting from interactions between aortic stenosis, intestinal angiodysplasia and acquired vWS-2A.
Aortic valve replacement rather than bowel resection leads to long-term resolution of anaemia and should be considered in severe cases. Early diagnosis and appropriate treatment of Heyde syndrome is essential but requires teamwork and liaison between different specialties.
Dr Abdelmugeet O.A. Hassan, MRCP UK, SCE, DGM (Geriatric Medicine) Specialty Doctor, New Cross Hospital

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...