Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]

Female genital mutilation (FGM) is an ancient practice dating back some 2,000 years to ancient Egypt and, although not explicitly mentioned is alluded to in the bible as a practice performed on Egyptian slaves. The practice of FGM is deeply embedded in certain communities and based on a range of motives, although the main reason relates to ensuring a woman is pure and chaste in preparation for marriage. FGM is prevalent in 28 African countries, parts of the Middle East and Asia (see Map). 1 FGM can lead to serious physical and psychological complications.
FGM is a form of abuse of women and children, illegal in the UK since the Female Circumcision Act of 1985, superseded by the Female Genital Mutilation Act of 2003, which extended the offence abroad and makes FGM punishable by up to 14 years in prison.2
With increasing migration, FGM is becoming more prevalent in the UK and clinicians need to be familiar with the issues and how to manage patients who have either undergone FGM or may be at risk of the practice. The Department of Health is gathering data regarding UK figures for FGM, although it is estimated that approximately 137,000 women and girls in England and Wales are survivors of FGM.3
This article looks at the background to FGM and aims to increase clinicians’ confidence in identifying and managing those who may be at risk of FGM or who have undergone this practice.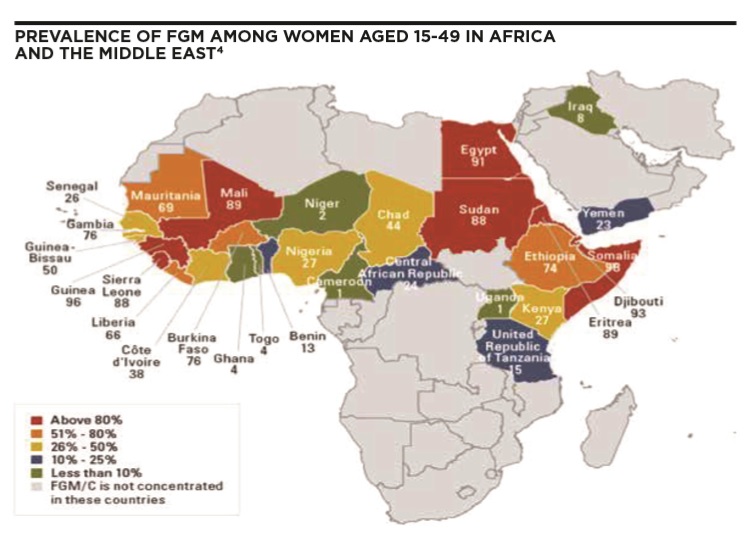
FGM is a practice deeply rooted in practising communities. Individuals rejecting FGM may be ostracised by their family and community. Motives for performing FGM vary between communities and reasons given can include:
Regarding religious reasons, there is no basis for the practice in religious texts of the Muslim, Christian or Jewish faiths.
Female genital mutilation (FGM) is also known as female genital cutting and female circumcision. The term FGM is generally applied in professional literature and will be used in this article.
Notwithstanding this, it is important for clinicians to ensure that they employ the utmost sensitivity in the terminology they use when communicating with patients, as the term “mutilation” carries negative connotations that may impact on a patient’s self- esteem. Most would prefer to be referred to as “survivors” rather than “mutilated”.
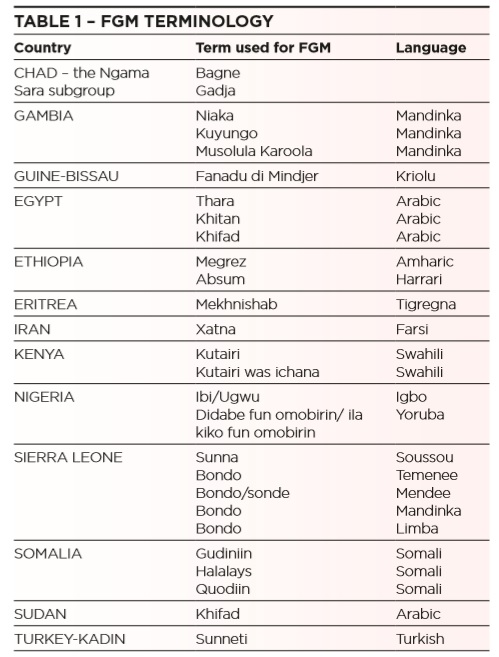
Furthermore, patients may be unfamiliar with the term female genital mutilation and it would be preferable to refer to “cutting”, “female circumcision” or to use colloquial terms (see Table 1).
Female genital mutilation comprises all procedures involving the partial or total removal of the external female genitalia or other injury to the female genital organs for non-medical reasons. The practice entails the removal and/or damaging of normal female genital tissue and can interfere with the normal function of the female body.
FGM confers no health advantages and may lead to physical and psychological complications, and in the worst cases death of a female who has had FGM and/ or her child due to complications in pregnancy and/or labour as outlined below.
FGM may be performed at any age, though the peak prevalence appears to be 5-8 years of age. However, it is important to note that FGM may be undertaken on much younger girls, including newborns, and many patients may not be aware that they have undergone the procedure. Furthermore, women may undergo the procedure after childbirth in order to restore the narrow vaginal opening created by type 3 FGM and widened in childbirth. This is called reinfibulation.

WHO has classified FGM into four types, and all are illegal in the UK. It may be difficult for a clinician to confidently diagnose the type of FGM performed, particularly in the case of type 4 FGM.
In some areas, such as Egypt, the practice is more medicalised with the use of sterile equipment and anaesthetic, yet long term physical and psychological complications may still arise.
Clinicians should note that patients may be unaware that they have undergone FGM and, even if they are, may not associate FGM with some of the complications they may be experiencing.
Early physical complications:
Late physical complications:
FGM is perceived by communities as an “act of love”, undertaken for the betterment of a girl’s life and to promote her acceptance into society as a chaste woman, in accordance with cultural precepts.
In the immediate aftermath of FGM, a woman or girl may be profoundly shocked by this practice having been arranged by loving parents and a caring community.
Consider the following case scenarios:
A school nurse contacts you to discuss her concerns regarding an 11 year old female pupil who has recently returned from a family trip to Ethiopia. She is spending long periods in the toilet and seems in some discomfort walking and sitting in class.
The practice nurse at your surgery comes to you with concerns regarding a young Nigerian woman she has just seen. She is three months pregnant but has not yet attended the surgery as she says she fears being examined and giving birth. Her sister’s labour lasted for three days, in which both her and her child nearly died.
Consider the probability of FGM bearing in mind the ethnic origin of these patients, the possible physical and psychological complications of FGM and how to manage these, as well as any risk to other females in the family and your safeguarding duties.
The 3 Cs questionnaire may assist when assessing whether FGM has been performed and to assess the risk of FGM:
A yes to at least one of these questions increases the risk of FGM and local safeguarding procedures should be followed.
If you do not ask the question, no-one will.
Women who have undergone FGM have comparable rates of PTSD as adults who have experienced abuse in early childhood, and 80% suffer from affective or anxiety disorders. 6
Psychological complications may include the following:
When considering a woman or girls risk of undergoing FGM, consider the following:
Indicators of immediate risk of FGM:
A girl or woman may:
The GP’s role is:
Regarding the physical consequences of FGM it may be necessary to refer a woman who has undergone the most extreme type of FGM, type 3, for deinfibulation, in order to widen the narrowed vaginal opening. Deinfibulation is a surgical procedure whereby the closed vaginal opening is opened.
With respect to safeguarding of children at risk of FGM, clinicians should promptly refer those at risk to social care, in accordance with safeguarding children principles and local policies and procedures.
Dr Sharon Raymond MBBS MRCGP NHS London FGM Steering Group

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...