Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]

The mortality and morbidity burden attributable to fragility fractures from osteoporosis is well established, yet less than one third of these patients receive bone-protecting treatments and interventions. In this article, Dr Madhavi Vindlacheruvu looks at how osteoporosis services can be rebuilt and reset following the Covid-19 crisis.

Osteoporosis is a disease characterised by low bone mass and structural deterioration of bone tissue leading to an increase in bone fragility and susceptibility to fracture. It is a progressive and asymptomatic disease that usually presents only after a fracture has occurred.
Over three million people in the UK have osteoporosis affecting one in two women compared to one in five men. The prevalence of osteoporosis increases with age from 2% at 50 years to more than 25% at 80 years in women. Women also experience increased bone loss after menopause.
Fragility fractures are extremely common in individuals aged over 50 years. Direct medical costs from fragility fractures are estimated to increase from £1.8 billion in 2000 to £2.2 billion by 2025. Less than one third of the patients experiencing the estimated 500,000 fragility fractures per year receive bone protecting treatments and interventions. Therefore, NICE recommend those who have experienced a fragility fracture should have their risk of fracture assessed.
Hip fracture is the most common reason for admission to orthopaedic wards with an estimated UK annual incidence of 101,000 in 2020. It is usually caused by an osteoporotic fragility fracture in an older person with osteoporosis and osteopenia.
Hip fractures are associated with high mortality; 6.7% in the first month and approximately 33% at 12 months. This is in part because many of these people have other long-term conditions or may be living with frailty, rather than the hip fracture itself.
Up to 75% of patients are admitted from home and approximately 10–20% of those will move to institutional care. Identifying patients in a systematic way could prevent up to a quarter of all hip fractures, which equates to almost 20,000 hip fractures a year.
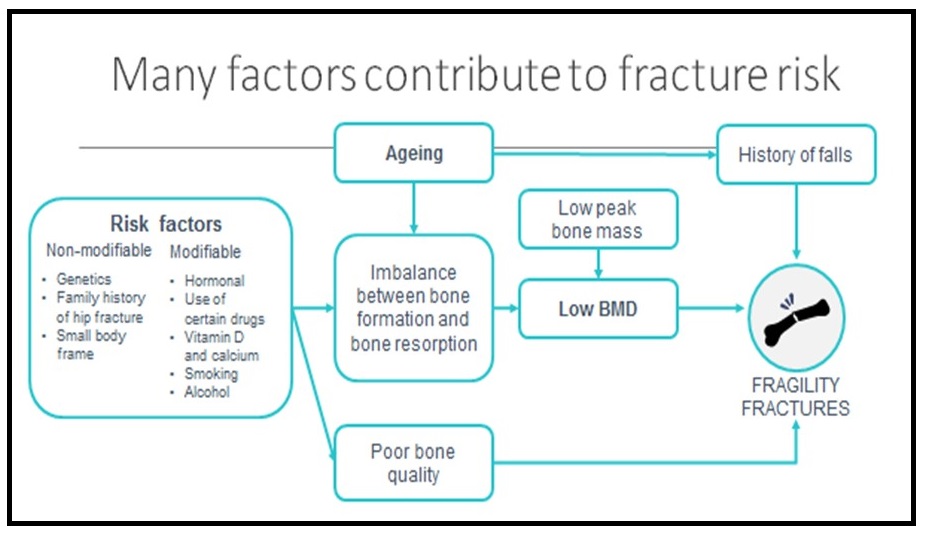
Fracture risk assessment tools should be used to predict fracture incidence over a period of time and help in decision-making to identify who may benefit from treatment.
Identifying people living with frailty is also a key intervention in the prevention of falls. NICE recommends use of the validated electronic Frailty Index (eFI) tool to identify people who may be living with frailty.
People at risk of fragility fractures include:
This tool can be used for people aged 40–90 years, either with or without bone mineral density (BMD) values. It is based on age, body mass index, fracture history, sex, smoking status, alcohol intake, corticosteroid use, femoral neck BMD and parental history of hip fracture. The tool calculates the 10-year probability of hip fracture and the 10-year probability of a major osteporotic fracture such as clinical spine, forearm, hip or shoulder fracture.
This tool can be used for people aged 30–99 years and cannot be used with BMD values. It is based on age, body mass index, family history, medical history, sex, ethnicity, smoking status, alcohol intake, parental history of hip fracture or osteoporosis, history of falls, antidepressants and corticosteroid use. The tool calculates risk of developing osteoporotic or hip fracture over 1–10 years.
A 81-year-old woman was seen in the emergency department after an unwitnessed fall. She went to put her dressing gown on and twisted and fell. She was immediately aware she had injured her ankle. There was no reported chest tightness, palpitations, breathlessness or dizziness at the time. She reported that ‘her balance that was off’.
For her falls risk assessment, the following was noted:
For her bone health assessment, the following was noted:
One third of over 65-year-olds will fall at least once each year resulting in 255,000 emergency admissions. The NHS RightCare pathway focuses on falls and fragility fractures. Commissioners who are responsible for falls and fragility fractures in their population should focus on three priorities for optimisation:
They should also ensure that schemes to deliver the higher value interventions are in place. This includes targeted case-finding for osteoporosis, frailty and falls risk, strength and balance training for those at low to moderate risk of falls, multifactorial intervention for those at higher risk of falls, and fracture liaison service for those who have had a fragility fracture.
The National Falls Prevention Coordination Group (NFPCG) and Public Health England recommend strength and balance exercise programmes for the majority of older people with a low to moderate risk of falls.
Strength and balance exercise programmes have been proven to be effective in primary and secondary prevention of falls and non-vertebral fractures in older people. These programmes have shown greater efficacy in patients who have a history of recurrent falls or who have a balance/gait deficit. For programmes to be effective, they must consist of at least 50 hours in total delivered at a minimum of two hours per week.
Fracture liaison services (FLS) can sit within primary or secondary care and are tasked with defining pathways for the identification of patients. They should:
The Fracture Liaison Service Database (FLS-DB) is a clinically-led, web-based national audit of secondary fracture prevention in England and Wales commissioned by the Healthcare Quality Improvement Partnership (HQIP) as part of the Falls and Fragility Fracture Audit Programme (FFFAP).
It is a continuous audit that measures primarily against NICE technology assessments and guidance on osteoporosis, and the Royal Osteoporosis Society (ROS) clinical standards for fracture liaison services (FLS). The annual FLS-DB report in 2020 indicated that FLS need to reach out to primary care in order to improve service delivery.
Quality improvement (QI) in osteoporosis care is required to:
Patients with osteoporosis should be advised of lifestyle changes that may improve bone health, such as taking regular exercise, eating a balanced diet, stopping smoking, and reducing alcohol intake. Pharmacological treatment includes calcium 700mg/day, vitamin D 800iu/day, antiresorptives and anabolics.
The population/individual mortality and morbidity burden attributable to fragility fractures is established and substantial treatment gaps still exist. Risk assessment is well validated, and widely incorporated in treatment guidelines. Secondary preventive strategies are well designed, widely available and cost-effective. A pragmatic approach is often required to account for frailty, falls risk, adherence to treatment, potential side effects and life expectancy.
Dr Madhavi Vindlacheruvu, Consultant Orthogeriatrician, Addenbrooke’s Hospital, Cambridge.
GM editorial team
This article is based on a presentation given at the GM Conference: Health and Ageing in a post-Covid NHS

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...
