Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]

Primary care manages most insect bite consultations but GPs are under pressure to reduce antibiotic prescribing and resistance rates. A survey by a subgroup of the RCGP overdiagnosis group examined current practice in insect and tick bite management. Two librarians undertook a literature review of studies in this area.

Primary care manages most insect bite consultations but GPs are under pressure to reduce antibiotic prescribing and resistance rates. A survey by a subgroup of the RCGP overdiagnosis group examined current practice in insect and tick bite management. Two librarians undertook a literature review of studies in this area.
Abstract
Introduction
Method
Results
Summary
References
Method: An online survey of a group GP members and their colleagues, combined with a literature search, resulting in 180 GP responses.
Results: Most GP respondents did not use a reference resource. In prevention, 61% recommended insect repellents, 31% advised on physical prevention. GPs mainly considered comorbidities, limb condition and systemic signs, with length of time of reaction in secondary infection assessment. Most GPs saw infected insect bites in the last year, with size of reaction and spreading erythema considered additional diagnostic helpers. Referral to secondary care was rare. 31% of GPs undertook investigations in the last 12 months, Lyme disease was the most common indication. Rates of infection and antibiotic prescribing were not available in literature review, but GPs’ reported prescribing followed national guidelines.
Conclusion: There is little published on primary care management of insect bites, almost all are managed in primary care and no comments on appropriate or inappropriate antibiotic prescribing can be made. As allergic, inflammatory and infected reactions can be difficult to differentiate, GPs use generic considerations of comorbidity and systemic signs.
Public Health England claims that one in five GP antibiotic prescriptions may be inappropriate. It is not possible to support this in insect bite management, specific coding to provide clear evidence is required. Increased research to help discriminate allergy, inflammation and infection in primary care would support better decision making.
The overdiagnosis group is an interest group of the Royal College of General Practitioners (RCGP) and is open to GPs, other health care practitioners (HCPs) and lay members. It is an informal email discussion group with a desire to prevent overdiagnosis, over-medicalisation, inappropriate interventions and therapy use.
Primary care management of insect bites and discussion of associated antibiotic prescribing occurred during the hot summer of 2018. Almost all insect bite consultations are managed in primary care, but there appears to be little published evidence on insect bite practice, although Francis et al1 demonstrated that UK GP practice prescribing of flucloxacillin between 2004 – 2013 had increased over time and increases in the summer months. Their data showed 96,000 prescriptions for flucloxacillin over this time period, generated by consultations specifically coded as ‘insect bite’. This is probably a gross underestimate, as the authors discuss, because infected bites might be labelled as cellulitis, non-specific rash or non-coded (i.e. a non-specific consultation title applied).
In addition, a study reported that up to one in five antibiotic prescriptions in general practice may be inappropriate.2 A subgroup was formed to investigate current insect bite management, looking particularly at four topic areas:
This study is not about acute anaphylaxis or severe allergic reactions; it is not about vector transmitted illnesses, apart from Lyme disease, but about day- to- day insect bites, largely from the UK, with which people present commonly to GPs. This is the first large scale publication on GP practice of insect bites to our knowledge.
There are two parts to the study, a literature review of the ‘risk of bacterial infection, cellulitis or sepsis after insect or tick bites for people in the UK’, and a survey of GPs on ‘usual’ management of insect bites in primary care. Both were carried out between September – December 2018.
Literature review:
The research question was refined into three areas:
Databases used were AMED, BNI, CINAHL, EMBASE, HBE, HMIC, Medline, PsycINFO, PubMed, Google Scholar and Google with citation searches of key articles.
Search terms included: UK, Lyme disease, Borrelia, tick bite, insect bite, bacterial infection, sepsis, antibiotic.
Survey of ‘usual’ GP practice in presumed insect bites:
Four key authors DD, CE, KH and JW created a survey based on the four topic areas above, arising from the group’s email thread. They defined and agreed questions. Apart from demographic questions, most questions asked for free text responses to capture qualitative realistic primary care practice and deter leading responses. This was available on Survey Monkey (appendix 1) from 22nd September to 15th November 2018 (54 days), with an estimated completion time of 10 minutes using 17 main questions.
Members were invited to share the survey with other clinicians by email link. The full results were shared amongst the clinical authors and selected for ‘GP only’ responses prior to analysis, as there were only small numbers of other clinicians. The GP respondents are overwhelmingly based in the UK, but a small number may be practicing abroad. Data extraction and initial analysis was undertaken by JW and L-J S, independently and then rechecked and discussed in the group to reconcile disparities, before finalising. The four key authors met and each GP was allocated one of the topic areas. Drafts were distributed to the wider author team for comment, improvement and agreement, and any discrepancies in data or analysis reviewed. Results are presented to the nearest percentage integer and as percentage responses from the number of GP respondents answering that question.
In UK primary care the rates of bacterial infection, cellulitis or sepsis after an insect bite were not available and there were no clear studies on rates of antibiotic prescribing after insect or tick bites. There was a lack of good quality, relevant studies for antibiotic usage, and those that were available focused largely on tick bites and Lyme disease.
Many studies were individual case reviews. This accords with a recent Cochrane Review (2016) on Lyme disease3 which pointed out the lack of valuable studies in this area. There was evidence for increasing incidence of Lyme disease, though still low compared to Europe and the USA, but there was no data on complication rates from tick bites. However, results highlighted that certain antibiotics, like doxycycline, appear to have a positive influence on various comorbidities associated with tick bites, especially in acute cases. A Norwegian study of three different antibiotics for adults with erythema migrans rash showed that of 180 patients, none developed Lyme borreliosis at 12-month follow up.4 Some further references are used within the discussion below.
GP estimates of insect bite workload and reasons for patient attendance
In total there were 199 responses of whom 180 were qualified GPs. Respondents were filtered to analyse qualified GPs’ responses only.
The 180 GP respondents were an experienced group; 41% had over 25 years of experience in practice, 26% had 15-25 years, 19% had 5-15 years and 13% had 1-5 years.
All respondents had managed insect bites in the previous 12 months, with estimated numbers ranging (to nearest 5) from less than 5 bites to 100 bites. The modal number was 5 bites per annum (pa) for 32% of GPs with 51% of GPs estimating 10-20 cases pa.
GPs selected from a fixed list of options why they felt patients attended in the last 12 months; more than one response was possible. 82% thought patients attended at times due to concerns about infection, 70% due to concerns due to severity of reaction, 41% due to concerns about length of time with reaction, 36% thought attendance was suggested by another HCP, 28% due to patients having previously been prescribed a medication for an insect bite, 25% for reasssurance,18% for general management advice, and 12% felt they had met patients for general management advice before holidays.
Prevention of insect bites
GPs were asked whether they recommended home or over the counter (OTC) remedies to prevent insect bites. There were 158 respondents and 243 responses given. Over half the respondents (61%) recommended some form of insect repellent (where types of insectides were stated N,N-Diethyl-meta-toluamide (DEET) was the most common recommendation). There were a dozen other products mentioned, some proprietary, including ‘Jungle Formula’ (contains DEET), ‘Citronella’ products and ‘Avon’ cream. 31% of respondents gave advice about clothing and nets to physically prevent bites. 7% of GPs would refer on to the practice nurses for advice.
Only one GP offered a practice website travel link. When asked if GPs had a useful resource in insect bite management for themselves 56% said they did not, DermNet NZ5 was the most commonly mentioned (7% of GPs).
Usual practice in non-infected and infected insect bites
Insect bites are not uncommon and 88% of 158 GP respondents felt confident in management (63% quite confident and 25% very confident). In distinguishing ‘usual’ bite reactions from cellulitis, 73% of GPs felt confident (63% quite confident and 10% very confident).
GPs were asked to list their top six factors they used in assessment. There were 160 respondents with 846 responses, of which 98 were too vague to analyse, leaving 758 responses. The top features GPs used were systemic symptoms and signs (72% of GPs), time from bite or time relating to speed of spread (60%) and patient comorbidities (47%).
Comorbidities specifically mentioned were diabetes mellitus, immunocompromise including chemotherapy or steroid treatment, extremes of older and younger ages, conditions affecting the local skin such as lymphoedema, eczema, peripheral vascular disease. Also mentioned but by less than 30% of GP respondents were itch, redness (26%), size, swelling, pain, heat, discharge, site, number, lymphangitis, previous reaction and Lyme disease risk.
71% of 161 GP respondents reported seeing infected insect bites in the previous 12 months, and clinical skills were similar to non-infected assessment. There were 539 responses from 147 respondents. Systemic features (78% of GPs), particularly pyrexia (43%), comorbidities or local limb condition (59%), and worsening reactions with spreading erythema after expected time to improvement (33%) were main considerations. The other features as in general assessment, except for itch, were also commented on. Only 6% of GPs mentioned pressure to prescribe from patients.

Asked about the natural history of ‘usual’ insect bites, 72% of 170 respondents felt that a normal reaction would reach maximal size at 2-3 days with a range from 1-7 days. It would then take 10-14 days to resolve (modal figure for 54% of GPs) with a range of 2-28 days given.
Of 132 GP respondents; 35% of GPs said they did not routinely prescribe for non-infected bites; 45% would sometimes prescribe an antihistamine and 22% sometimes prescribed hydrocortisone cream.
Asked specifically what they suggested or prescribed for non-infected bites if indicated, 88% of 132 GPs suggested OTC or prescribed oral antihistamines, 39% a steroid cream (usually hydrocortisone cream), 30% ice or cold compress, 31% gave safety advice on expected progress and when to return (safety-netted) and reassured, 13% suggested limb elevation, 8% analgesia, 7% local antihistamine cream and a few GPs offered a variety of additional strategies: menthol cream, Eurax, antiseptics, non-steroidal anti-inflammatory (NSAI) gel, calamine, emollients, drawing a line around the reaction to see if it is expanding, patient information leaflet and oral non- steroidal ani-inflammatory (NSAID) drug.
Vaccination (including tetanus status) was not routinely considered by 74% of GPs.
The majority (69%) of 173 respondents had not investigated insect bites in the previous 12 months. Of the 31% that had investigated, most investigated for Lyme disease (57%); the remainder were occasional tests for FBC, CRP, diabetes, Malaria, Weil’s serology and a swab.
When prescribing antibiotics for an infected bite, 80% of respondents prescribed flucloxacillin. Other occasional antibiotics were co-amoxiclav, phenoxymethylpenicillin, amoxicillin and topical fusidic acid, but macrolides did not feature first line. Doxycycline was mentioned in the context of suspected Lyme disease. There were two referrals (one to dermatology outpatients and one discussion with an infectious disease specialist). Only five GPs reported any experience of admission for patients: cellulitis (3), lymphangitis (1) and blistering, but due to possible pemphigus (1).
Consideration and influence of Lyme disease (from tick bites) as a diagnosis
GPs did not think that patients presented due to Lyme Disease concerns and 12% stated they usually specifically checked for Lyme Disease, 19% considered geography, and 10% would take foreign travel or tick risk into account, asking where the bite had been sustained geographically (eg. if while playing in woods, or a park).
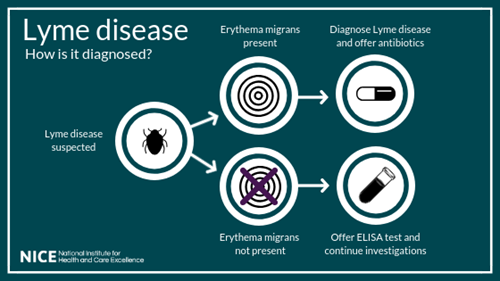
However, when GPs were specifically asked if they ever considered Lyme Disease as a factor, 95% of 144 respondents had, 17% of respondents would ask specifically, 26% would ask or look for tick bites and 31% mentioned characteristic rash (erythema migrans). Knowledge about how to diagnose and treat Lyme Disease was varied (30 responses), with some confusion on the role of serology and when blood tests should be done. There were also varying responses on treatment of Lyme Disease, with 28 respondents mentioning tetracycline antibiotics, and another 23 mentioning antibiotics non-specifically.
Most insect bite presentations are dealt with in primary care, with a wide variation in estimated numbers seen, rare referrals and admissions, so little secondary care input.
Whilst GPs felt that patients presented due to concerns about infection and duration of reaction, about 36% thought other clinicians created inter-referrals and possibly pressure for antibiotic prescription, this is likely to be an increasing primary care pathway. GPs had no well- used reference resource.
GPs assess patients for systemic features of infection, comorbidities and local factors before deciding whether an insect bite is infected. These are non-specific to insect bite practice and reflect the paucity of discriminators in this area. Wheal and flare versus macular erythema were not major reported discriminators. As GPs are not seeing ‘usual’ self-limiting bites, they are managing bites that patients have concerns about, reactions are likely to be atypical, making distinction between allergy, inflammation and infection difficult.
When antibiotics were prescribed, GPs chose flucloxacillin in accordance with national guidelines,6 GPs did not mention dual antibiotic use or concomitant oral and topical antibiotic prescribing or delayed prescriptions. Lyme disease (from a tick bite) was included in the survey because its testing has increased in the UK over recent years and with publication of recent NICE guidance.7 Our literature search estimates 2-3,000 cases of Lyme disease in the UK each year8 and in England and Wales just under two people per 100,000 are infected with Lyme disease.9
Cases with an erythema migrans rash do not require testing7 and negative tests are not included in statistics, so real rates of tick bite diagnoses are unknown. Literature tends to revolve around case reports (e.g. Lyme carditis10). Most GPs had not investigated insect bites in the last 12 months (69%) but of those that did over half tested for Lyme Disease. Awareness of tick bites appears to be high in GP insect bite consultations, but knowledge of how to diagnose and treat Lyme Disease was variable, consistent with the relatively recent guidance production.7 NICE recommended treatment for Lyme disease is based on identification of erythema migrans and suggests 3 weeks of oral doxycyline for suitable population groups.
Strengths and limitations
This study relates real-time general practice to current literature on insect bite practice. This aligns with Rapport and Braithwaite’s11 Fourth Research Paradigm which recognises research methodologies, both quantitative and qualitative, which are collected ‘on the hoof’ often using social media, to improve understanding. It surveys a large number of experienced GPs and is an insight into current practice.
The frequent use of free text led to rich descriptive responses but increased disparities at coding, which were then reconciled, both a strength and a weakness and data could only be interpreted at times at a pooled, thematic level. Two questions were not analysed because of perceived weaknesses in wording at analysis. The question on vaccination was poorly worded as it did not distinguish foreign and UK requirements.
Recall bias also limits the validity of responses. Sampling bias, inherent in membership of the group, means that results may not be generalisable to all other GPs. There is no data on sessions worked, out of hours experience and GP’s geographical location so no differentiation between urban and rural general practice. We did not capture consultations with other primary health care clinicians.
Comparison with existing literature
GPs use no standard information resource, occasionally mentioned was DermNet NZ,5 which is used for any dermatological condition. Several sites offer clear advice to patients about prevention using physical and insecticidal means e.g. Travelhealthpro,12 Fit for Travel13 and Bug Off!14 and promotion of one site for GPs might be useful. DEET was most mentioned in prevention and GPs could consider physical protective advice more often. There is evidence of effectiveness of DEET and Picaridin as insecticides, with DEET being most effective for the longest time at the higher 50% concentration15,16,17,18, with few cases of serious toxic effects ever reported. Citronella products are of less efficacy (shorter length of time of protection compared to Picaridin or DEET).19
There does not appear to be any evidence for some of the individual suggestions of turmeric, garlic, vitamin B, Marmite and mint tea and there was no evidence for ultrasonic devices, suggesting personal experience may influence GP advice.
In uncomplicated bites CKS20 has a scenario exemplar for primary care management, recommending removal of any sting or tick if present and suggesting cold compress. If itch is a problem oral antihistamines or topical hydrocortisone cream, may reduce itching but there is no good quality evidence for this. This accords with our own survey of GP practice. Bug off!14 suggests cold compress, local antihistamine or local anaesthetic. Few GPs mentioned antiseptics in our survey, but these are suggested on public sites12,13 but have little evidence base. GPs have no near patient test for infection, with recommendations largely based on medical culture and expert opinion.21
In secondary care classification of soft tissue infections is made.22 This is not commonly recorded in primary care but features of cellulitis with or without comorbidity and consideration of systemic features are key in this staging and has been recently incorporated into primary care antibiotic tables.6 Features of severe pain and tenderness were not frequently mentioned in distinguishing rare complications like necrotizing fasciitis. Panton-Valentine Leucocidin is mentioned in national primary care antibiotic prescribing tables6 as are tick, but not insect, bites.
Three-quarters of antibiotics are prescribed in UK primary care, a study of acute antibiotic prescriptions over a 7% sample of the UK population found that 30% of the population receive at least one antibiotic prescription per year.23 All acute antibiotic prescriptions for ‘bites’ accounted for 1% of coded entries (many consultations were not coded) and these bites may not have been due to an insect.
Patients are not always sure if they have been bitten or stung, by what sort of insect or even an insect at all. Insect bites may really be contact reactions to vegetation, bites may occur from a variety of UK or foreign insects, ticks, spiders etc. and reactions can vary from small red reactions to multiple or large areas, some as blisters or papules, some painful, and most itchy. Understanding what constitutes a normal pathophysiological response to an insect bite, how long this takes to resolve, the concept of distress tolerance and advice on signs of infection would be helpful for GPs and coworking HCPs.
The simple step of drawing a pen line around the limits of erythema may empower patients and links with aspects of safety netting advice but was rarely mentioned in the survey. The RCGP Overdiagnosis Group has identified a clinical area that lacks a solid evidence-base and summarised current practice and knowledge. This helps define areas for future research, but evidence is not robust enough to refute or agree on optimal antibiotic use in insect bite consultations. GPs manage almost all insect bites; it is rare for cases to reach secondary care. Prescribing generally aligns with national guidelines so advances in what to prescribe are not required as much as how GPs make decisions on when to prescribe. We found no literature information on this area in primary care and have related current GP decision making.
Appendix 1
SURVEY QUESTIONS ON INSECT BITE PRACTICE

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...
