Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Dementia is a devastating illness that leads to a progressive decline in a person’s cognition and functioning. Patients frequently experience a wide array of behavioural and psychological symptoms, including agitation and aggression. These symptoms can be extremely distressing to patients and those who care for them. Antipsychotic medications have been the mainstay of pharmacological treatment and are used to treat these in patients with dementia in both the community and in hospital. However, recent studies have shown an increased risk of morbidity and mortality with long-term use.
Dementia describes a clinical syndrome that leads to a progressive decline in multiple areas of functioning that include memory, reasoning and communication, leading to a deterioration in the person’s ability to carry out everyday activities independently. It is a progressive disease caused by structural and chemical changes in the brain. The causes include Alzheimer’s disease, vascular dementia, dementia in Parkinson’s disease, lewy body dementia and frontotemporal lobe dementia.
The Alzheimer’s Research Trust stated in its report, Dementia 2010, that there are currently 820,000 people with dementia in the UK.2 This represents approximately 1.1% of the population, with the incidence and prevalence increasing exponentially with age. Although dementia is predominantly a disorder of later life there are at least 15,000 people under the age of 65 years with dementia in the UK.
In addition to cognitive and functional decline, patients commonly experience the diverse range of behavioural and psychological symptoms (Box 1).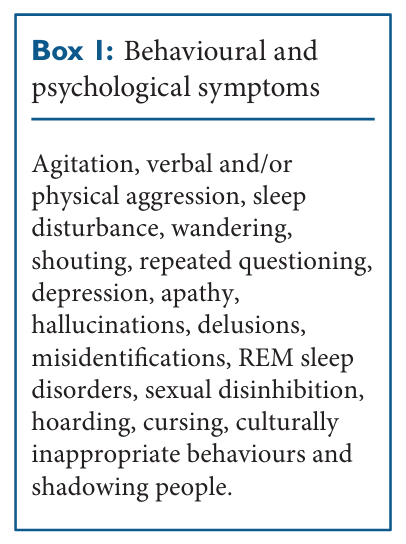
Behavioural and psychological symptoms can occur at any point in the illness, often causing distress for the patient and those who care for them whilst presenting significant management challenges for healthcare professionals. These symptoms are common in dementia, with a prevalence of 60% to 80% and a cumulative risk of 90% during the course of the illness.4 These symptoms are often the precipitating factor for institutionalisation.
There is an unmistakable need to treat these symptoms with the objective of alleviating the suffering caused, reducing the risk when a patient becomes physically aggressive and reducing early institutionalisation. Antipsychotic medications have been the mainstay of psychopharmacological treatment for behavioural and psychological symptoms of dementia over the past few decades.
However, in 2004, the Committee for Safety of Medicines (CSM) issued safety concerns regarding the use of risperidone and olanzapine in dementia due to an increase in cerebrovascular events. This led to an increase in evidence suggesting that antipsychotic medications present significant risk, which may outweigh the benefits.
Antipsychotic medications have been used since the 1950s and are mainly licensed for use in schizophrenia and bipolar disorder where there is evidence of psychosis. The first-generation of these medications, known as “typical” antipsychotics, act predominantly by antagonising dopamine receptors. These have been superseded by the second-generation “atypical” antipsychotics, largely due to a more favourable side-effect profile and a perceived relative safety advantage.
Elderly patients are at increased risk of side effects, including postural hypotension, dyskinesias and extrapyramidal effects, due to frailty, comorbidities and polypharmacy. These adverse effects can lead to an increased rate of falls and their devastating effects on a patient’s physical and psychological wellbeing. With one exception, the use of antipsychotics is unlicenced for the treatment of behavioural problems in dementia.
Risperidone has a licence in the UK for the short-term management of persistent aggression in patients with moderate-to-severe Alzheimer’s dementia unresponsive to non-pharmacological approaches where there is risk of harm to self or others lasting for a period of six weeks. Nonpharmacological approaches include environmental, medical, nursing and social interventions such as restructuring the care plan, person-centred care and treating physical issues such as pain and constipation.
This number is likely to be an underestimation due to the fact that a significant number of patients with dementia will not have a formal diagnosis. The Department of Health report ‘The use of antipsychotic medication for people with dementia: Time for action’ made a conservative estimate that one quarter of people with dementia in the UK are on antipsychotic medication at any one time equating to 180,000 individuals.
In 2004, a Medicines and Healthcare products Regulatory Agency (MHRA) review considered four randomised controlled trials of risperidone and found that there were 33 cerebrovascular adverse events with risperidone versus eight with placebo. The MHRA also assessed olanzapine and found a similar increase in the risk of stroke and a two-fold increase in all-cause mortality.
As a result of the MHRA review, the CSM advised that olanzapine and risperidone should not be used for the treatment of behavioural symptoms in dementia due to clear evidence of increased stroke risk in elderly patients with dementia. They recommended that if risperidone was used in the management of acute psychosis in patients with dementia, it should be short term and under specialist advice.7
Schneider et al conducted a meta-analysis in order to establish mortality and morbidity risk and found that there was an increased risk of death with atypicals (OR=1.54; 95% CI 1.06– 2.23, p=0.02) and an increased risk of stroke (OR=2.13; 95% CI 1.20–3.75, p=0.009).8
Another meta-analysis investigated the efficacy and adverse effects of atypical antipsychotics in dementia and found sufficient evidence for symptomatic efficacy with risperidone and aripiprazole. It was found that olanzapine was not associated with efficacy and that there was no evidence for the use of quetiapine.9 Ballard et al conducted a review of sixteen randomised, placebo-controlled trials where dementia and psychosis and/ or aggression were assessed. Nine of these had sufficient data to contribute to a meta-analysis.
They found evidence to suggest that risperidone and olanzapine are useful in reducing aggression and risperidone reduced psychosis, but both are associated with serious adverse cerebrovascular events and extrapyramidal symptoms. The authors concluded that neither risperidone nor olanzapine should be used routinely to treat dementia patients with aggression or psychosis unless there is severe distress or risk of physical harm to those living and working with the patient.10
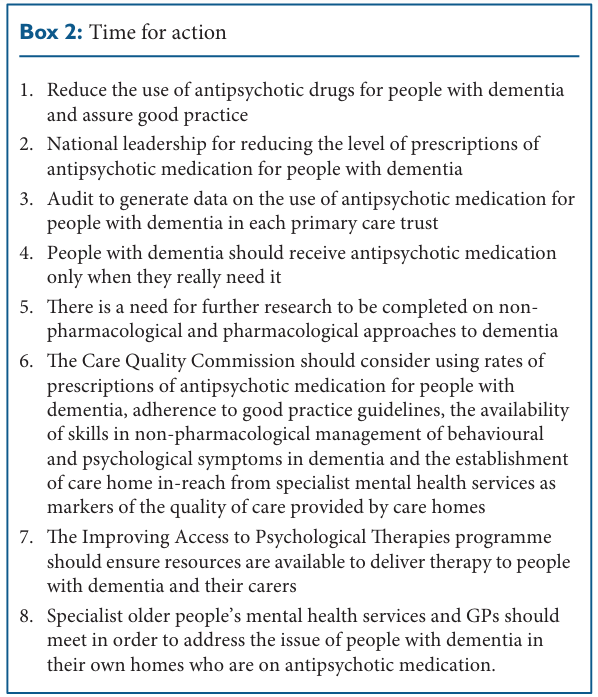
‘The use of antipsychotic medication for people with dementia: Time for action’,1 states that there is an evidence base that proves that antipsychotic medications are being used too often in people with dementia with detrimental effects. The report made several recommendations in order to lead to effective action, some of which are summarised in Box 2.
Prevalence of use There has been increasing concern over the number of patients with dementia prescribed antipsychotic medications. Fossey et al found that 48% of patients with dementia in 12 nursing homes were prescribed antipsychotic medication5 and a recent report from IMS Health,6 a provider of pharmaceutical market information, suggested that 20.3% of prescriptions for the treatment of people with the recorded diagnosis of dementia included an antipsychotic medication.
The report highlighted that the use of antipsychotic medication in dementia is an indication of a general cumulative failure in health and social care systems to develop an effective response to challenges posed by dementia. The recommendations made in the report intend to reduce the use of antipsychotic medication in dementia to a level where the benefit gained will outweigh the risk, including 1,800 extra deaths and 820 serious adverse events, and assure that patients are being managed safely and effectively.
The evidence for antipsychotic medication is best for physical aggression and not verbalisations or wandering. Risperidone has a short-term licence in the UK for use in persistent aggression resistant to non-pharmacological approaches. Any other prescription would be used out of licence and should, wherever possible, involve a discussion with the patient’s family if the patient lacks capacity.
Aripiprazole has the second-best evidence but use would be against manufacturer’s advice and there is little evidence for the use of olanzapine and quetiapine. Keeping in mind the cautions previously mentioned, antipsychotics in order of evidence base for effectiveness are: risperidone, aripiprazole, olanzapine and quetioapine.
All prescriptions for antipsychotic medications for people with dementia should be time limited due to the significant risk of morbidity and mortality with long-term use. Practice is evolving and many prescribers are giving stop dates of six weeks to three months on initiation, with a view to restarting if the behavioural or psychological symptoms recur.
In all prescriptions, it is important to document that nonpharmacological methods have been tried and that the risk of non-treatment outweighs the risk of treatment. Wherever practical and timely, this should be done under the Mental Capacity Act if the patient lacks capacity. This advice appertains to the use of antipsychotic medications for people with dementia and not a primary psychosis.
The use of antipsychotic medications to treat behavioural symptoms in patients with dementia with or without nonpharmacological interventions is common despite evidence of only moderate efficacy and serious adverse effects. Evidence suggesting that the risk of stroke and death is notably increased has led to recommendations against the use of antipsychotic medications in dementia for behavioural and psychological symptoms.
Good practice guidelines recommend psychological and environmental management approaches first line, which Fossey et al5 found led to a significant reduction in the requirement for antipsychotic medication for patients with dementia in nursing homes. Medication may be required to reduce severe distress or risk of physical harm to those living and working with the patient. In these circumstances, risperidone has the best evidence and is licensed for physical aggression and psychosis and should ideally be a short-term prescription with an automatic stop date.
Dr Nicola Smith, Foundation Trainee Year 2 in Psychiatry, Victoria Centre, Swindon
Dr Simon Manchip, Consultant in Old Age Psychiatry, Victoria Centre, Swindon
Dr Nicola Smith has no conflicts of interest. Dr Simon Manchip has lectured for and sat on advisory boards for Lundbeck, Jannsen, Eisai, Shire and Pfizer

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...