Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Prostate cancer is the second leading cause of cancer death in men in the western world. Castrate resistant prostate cancer (CRPC) occurs when hormone therapy fails to arrest the growth of prostate cancer; death due to prostate cancer is a result of CRPC. Chemotherapy is used in the treatment of CRPC and has shown improvement in quality of life and a modest survival benefit. In this review we discuss new biological treatments as well as the role of radiotherapy and radionuclides in the treatment of CRPC.
Prostate cancer is the commonest male cancer and accounts for 25% of all new cancers in men in England and Wales. In 2006, 35,515 new cases of prostate cancer were diagnosed in the UK. The lifetime risk of being diagnosed with prostate cancer is one in 10 for men in the UK, with the peak incidence at 70–75 years.1 The disease is a major clinical problem, not only because of its high rate of incidence and mortality, but also because of the severe morbidity associated with its advanced stages.
More than 95% of prostate cancers are adenocarcinomas, with rarer forms such as transitional cell carcinoma (TCC), small cell and lymphomas occurring much less frequently. For the purposes of this review, we will be discussing adenocarcinomas of the prostate.
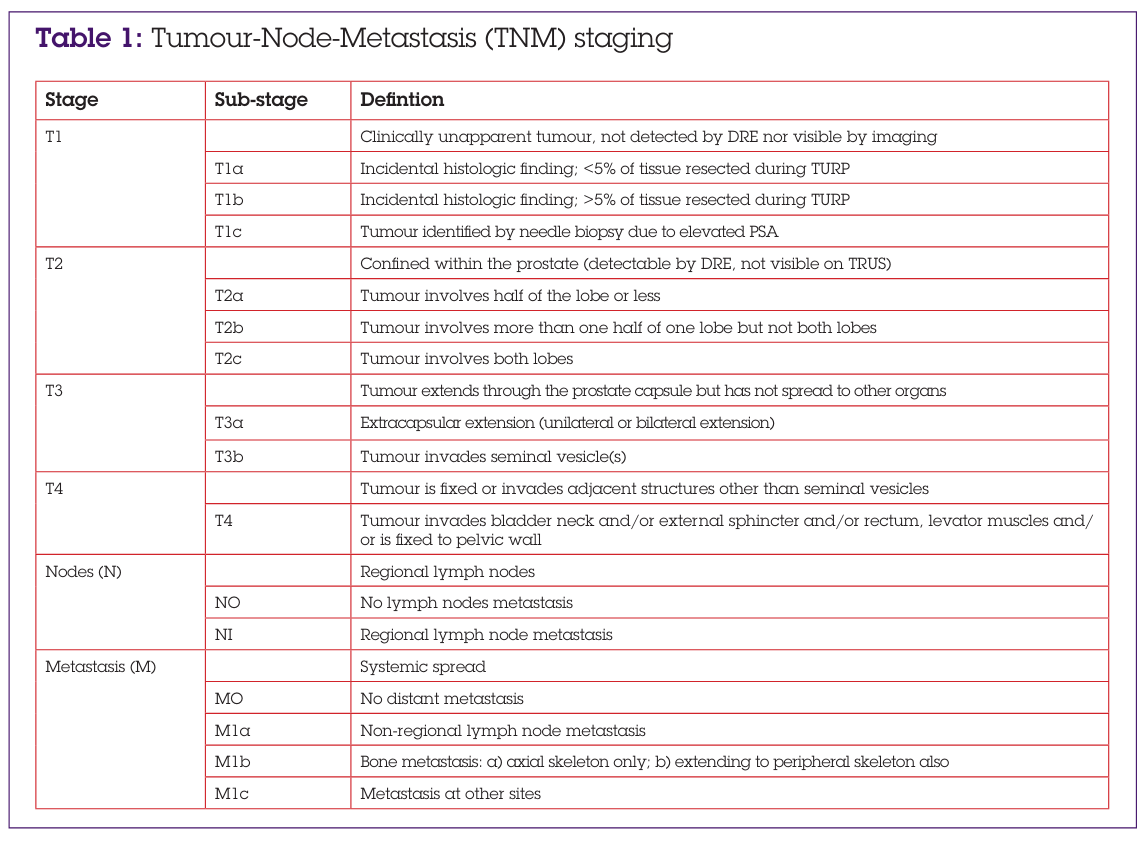
When a patient initially presents with prostate cancer, investigations—including prostate specific antigen (PSA), digital rectal examination (DRE), transrectal ultrasound (TRUS), biopsies of the prostate, and staging scans (MRI and bone scan)—are performed to evaluate the extent of spread of the cancer. Information obtained from the staging investigations can be used to classify the cancer as being “localised“, “locally advanced”, or “metastatic” (see Table 1).
The Gleason score is the most commonly used system of identifying the histological characteristics of prostate cancer. It is based on glandular architecture and the relationship of the glands to the stroma within the tumour.
A grade of 1 indicates a near-normal pattern, and grade 5 indicates the absence of any glandular pattern. The predominant pattern and the second most common pattern are given grades from 1-5. The sum of these two grades is referred to as the Gleason score, which can range between 2 and 10. It is now unusual to see Gleason scores of less than 6 because the lower patterns (1 and 2) are not thought to be cancerous.2 A Gleason score of 6 (or less) may be described as “well differentiated” as the cells appear similar to normal prostate tissue and these cancers are generally less likely to spread to distant sites. A Gleason score of 7 is considered to be “moderately differentiated”, and Gleason scores of between 8 and 10 are “poorly differentiated”. Cancers that are poorly differentiated are the most aggressive type and are likely to spread to distant sites.
With localised prostate cancer (cancer confined to the prostate: T1 and T2), the Gleason score and the PSA level are used together to determine the risk of the cancer spreading. “Low risk” tumours are when the PSA is ≤10 and the Gleason score is ≤6, “intermediate risk” tumours are those with a PSA of 10–20 and a Gleason score of 7, and high-risk tumours are when the PSA is ≥20 and the Gleason Score is ≥8. For all types of prostate cancer, choice of treatment is based on the patient’s stage of cancer, Gleason score, and the PSA level.
Before commencing treatment, doctors should discuss with the patients (and their families) the different treatment options available.
The aim of treatment for all localised prostate cancers is curative, but treatment used depends on the risk level. For “low risk” or “intermediate risk” cancers, the options include active surveillance, radiotherapy (external beam radiotherapy or low dose rate brachytherapy), surgery, or a combination of hormones and radiotherapy. Whilst all these treatment modalities differ in their toxicities, they have similar disease outcomes and the choice of treatment is largely made based on patient preference and performance status. Localised prostate cancer with high-risk features can be treated with either surgery or a combination of radiotherapy (external beam alone and/or high-dose rate brachytherapy) and hormones. Men with localised disease (when treated with curative intent) generally have a good long-term outcome.3
Locally advanced prostate cancer includes cancers that have spread outside the prostate (T3/T4) or those that have spread to the pelvic lymph nodes (N+). Cancers that have spread just outside the prostate (T3a /T3b) but have no evidence of lymph nodal involvement (N0) can be treated with curative intent with a combination of radiotherapy (external beam alone and/or high-dose rate brachytherapy boost) and adjuvant hormone treatment for two to three years. Cancers that have spread to adjacent organs (T4) or that have spread to lymph nodes (N+) are generally not curable. Based on the patient’s performance status, symptoms and preferences, he can be treated with hormone treatment alone or with watchful waiting.
The growth of most prostate cancers is stimulated by testosterone, and hormonal therapies that modify levels of testosterone or modify responses to it are standard treatment for men with metastatic disease (cancer that has spread to bones or other organs). The initial treatment for metastatic prostate cancer is hormone ablation therapy either by surgical castration (orchidectomy) or by medical castration with luteinizing hormone-releasing agonists (LHRHa) with or without antiandrogens (bicalutamide, flutamide). Hormonal therapies are initially effective in 80% of men with metastatic prostate cancer, but after around 18 months the disease can become unresponsive to hormone treatment and will progress.
Castrate resistant prostate cancer (CRPC) or hormone refractory prostate cancer (HRPC) occurs when hormone therapy fails to the stop the growth of prostate cancer. There is no universally accepted definition of CRPC. The disease can be considered castrate resistant when in the presence of castrate testosterone levels, androgen deprivation therapy or combined androgen blockade no longer controls the PSA (classified as a PSA ≥5, and two consecutive rises in PSA obtained at intervals greater than two weeks). Alternatively, there are symptoms or radiological evidence of progression. For example, patients with CRPC may present with symptoms that relate to local or metastatic progression, such as bone pain, haematuria, and urinary outflow obstruction, back pain due to ureteric obstruction, pelvic pain, lymphoedema or perineal discomfort. However, some patients may be asymptomatic.
For asymptomatic patients, PSA is the single best marker. But imaging modalities, such as bone scan, CT scan and MRI scan, are useful to detect metastases. The most common site for metastases is bone, followed by spread to the pelvic lymph nodes. Other sites of metastases (lung, liver, adrenals) occur less than 5% of the time. Brain metastases occur in approximately 1% of patients.
CRPC may still respond to agents such as oestrogens or corticosteroids that are postulated to work via the androgen receptor. Even when the disease becomes hormone refractory, the androgen receptor on the cancer cells can remain active and LHRH agonists are usually continued. This stage of prostate cancer is associated with substantial morbidity and mortality. There is no known curative therapy, so the goals of treatment are to improve quality of life, control symptoms and to ultimately lead to a survival benefit.
When men with prostate cancer develop biochemical evidence of castrate resistant disease, their treatment options should be discussed with a urological cancer multidisciplinary team (MDT). The management of the physical symptoms and psychological needs of men with metastatic prostate cancer need to draw on the expertise of an oncological and/or specialist palliative care opinion as appropriate. Based on the patient’s symptoms and fitness, local radiotherapy, hormones, chemotherapy or supportive care are the potential options.
Diethylstilbestrol is a synthetic oestrogen that can reduce the PSA level in men with CRPC, although the mechanism of action is not fully known. Low-dose corticosteroids can reduce the production of adrenal androgens in men by suppressing adrenocorticotropic hormone (ACTH) secretion from the pituitary gland. This effect can be achieved by physiological doses of corticosteroids such as dexamethasone, prednisolone or hydrocortisone.
Chemotherapy is usually given to men with CRPC who have symptomatic progression or asymptomatic men with metastatic disease and a rapidly rising PSA. The androgen receptor on the cancer cells can remain active and LHRH agonists are usually continued. The chemotherapy regimen licensed for these patients involves a combination of docetaxel and prednisolone. It is recommended for men with a Karnofsky performance status score of 60% or more. Karnofsky performance refers to the patient’s functional status, and a score of 60% or more indicates that the patient is able to care for himself with only occasional assistance (if any).
A three-arm trial (TAX327)4 comparing mitoxantrone and prednisolone, weekly docetaxel and prednisolone and three weekly docetaxel and prednisolone showed median survival of 14, 16 and 18 months respectively. Three weekly docetaxel led to an improved median survival of 2·4 months and improved rates of response in terms of pain, serum PSA level, and quality of life, compared with the other arms. Three weekly docetaxel/ prednisolone is now approved by the NICE5 guidance for prostate cancer. Treatment with docetaxel should be stopped at the completion of a planned treatment schedule of 10 cycles, or earlier in the case of severe adverse events, or in the presence of progressive disease as evidenced by clinical findings, laboratory criteria, or imaging studies. The results of this trial have recently been updated,6 and the survival benefit with three weekly docetaxel has persisted with extended follow-up. Median survival time was 19·2 months for three weekly docetaxel verses 16·3 months in the mitoxantrone arm (p=0·006) with respective three-year survival figures of 18·6% versus 13·7% in favour of docetaxel. This study has confirmed the benefits of docetaxel chemotherapy, but there is uncertainty about the optimum timing of treatment and about the patient subgroups that will benefit the most.
Radiotherapy is effective at relieving local symptoms such as bone pain, haematuria, urinary outflow obstruction, back pain due to ureteric obstruction, pelvic pain, lymphoedema, or perineal discomfort caused by local progression of prostate cancer.
Both radiotherapy and radioisotopes are very effective in palliating symptoms secondary to bone pain. A systematic review of 20 trials, reporting on 43 different radiotherapy fractionation schedules and eight studies of radioisotopes, showed complete pain relief at one month in 395 out of 1580 (25%) patients and at least 50% pain relief in 788 out of 1933 (41%) patients at some time during the trials.7
A study from The Bone Pain Trial Working Party showed that a single fraction of 8 Gy is as safe and effective as a multifraction regimen for the palliation of metastatic bone pain for at least 12 months. There were no differences in the time to experience improvement in pain, time to complete pain relief or in the time taken for pain to recur in the first 12 months from randomisation, nor in the class of analgesic used.8
Radionuclides are useful to palliate symptoms of bone pain due to metastases. Strontium-89 is a β-emitting radionuclide that preferably localises in areas of active bone formation and gives off its radiation directly to the cancer cells (areas of high osteoblast activity such as metastatic lesions). Strontium liquid is given as an intravenous injection. Evidence of pain relief is generally seen within seven to 21 days and sustained for three to six months. A repeat dose can be administered at three-monthly intervals if necessary. Strontium can cause bone marrow suppression and this should be carefully monitored.9
A study comparing patients with prostate cancer and painful bone metastases treated with local or hemibody radiotherapy or strontium showed no difference in median survival between groups. Both radiotherapy and strontium provided effective pain relief that was sustained for three months. Radiotherapy to a new site was required by 12 patients in the local radiotherapy group compared with two after strontium (p<0·01), although there was no significant difference between groups receiving hemibody radiotherapy (six patients) and strontium (nine patients).10 ><0·01), although there was no significant difference between groups receiving hemibody radiotherapy (six patients) and strontium (nine patients).10
Prostate cancer has a propensity to spread to the bones and the growth of the cancer cells leads to the destruction of bone tissue. In addition to their use in the management of hypercalcaemia, bisphosphonates also help to control bone pain. A meta-analysis, reviewing 10 randomised trials,11 showed a trend favouring bisphosphonates over placebo in the relief of pain from bone metastases and a reduction of skeletal events in men with prostate cancer. However, there was no statistically significant overall difference between the bisphosphonate group and the control group in terms of prostate cancer death, disease progression, radiological response or PSA response.
A placebo-controlled trial using third generation bisphosphonate, zoledronic acid 4mg administered every three weeks intravenously, demonstrated reduced skeletalrelated events (SREs) in prostate cancer patients with bone metastases. At the two-year analysis, treatment with zoledronic acid was found to significantly reduce the percentage of patients with at least one SRE compared with placebo (38% versus 49%, respectively; p=0·028). These events were defined as radiation for bone pain or to prevent pathological fracture/spinal cord compression; pathological fracture; spinal cord compression; surgery to bone; change in antineoplastic therapy). Zoledronic acid also significantly delayed the time to first SRE by around six months (median 488 versus 321 days; p=0·009). Pain scores were consistently lower in patients treated with zoledronic acid than those treated with placebo.12
Bisphosphonates may be considered for pain relief in men with hormone-refractory prostate cancer when other treatments (including analgesics and palliative radiotherapy) have failed. There is an ongoing clinical study called the “RIB” trial, comparing bisphosphonate treatment in the form of a single infusion of ibandronate to radiotherapy to see which approach is more effective at controlling pain from bone metastases.13
The endothelin axis plays a key role in the development and progression of advanced prostate cancer. Activation of the endothelin-A receptor (ETAR) by endothelin-1 (ET-1) is thought to promote several processes involved in tumour progression, through inhibition of apoptosis, promotion of angiogenesis and invasion and changes in skeletal biology associated with bone metastasis.
ZD4054 (zibotentan) is a specific ETAR antagonist. It is an oral compound that has been shown to be generally well tolerated.14 The most frequent toxicities are reported as nasal congestion, headache and peripheral oedema. A double-blind, placebo-controlled, randomised, phase 2 trial has shown that ZD4054 improves survival for CRPC patients with bone metastases The significant improvement in median overall survival for the ZD4054 treatment groups compared with placebo was 23·5, 24·5 and 17·3 months in the ZD4054 15mg, ZD4054 10mg and placebo groups, respectively. This drug is currently being investigated further in large international phase 3 studies.
Prostate cancer is often slow-growing and expresses many tumour-associated antigens, making it a feasible target for immunotherapy.
Sipuleucel-T is an investigational active cellular immunotherapy product designed to stimulate an immune response against prostate cancer. The safety and efficacy of sipuleucel-T was evaluated in two identically designed, randomised, double-blind, placebo-controlled trials (D9901 and D9902A) conducted in men with advanced prostate cancer. Patients randomised to sipuleucel-T demonstrated a 33% reduction in the risk of death.15
Denosumab is a monoclonal antibody that inhibits osteoclast mediated bone resorption in bone metastases from solid tumours. A phase II trial comparing denosumab and IV bisphosphonate showed denosumab reduced markers of bone resorption and reduced the incidence of SREs. This evidence suggests that denosumab may provide a new alternative for the prevention of bone resorption and resulting skeletal complications in patients with prostate cancer.16 The results of ongoing clinical trials are awaited.
Tumours frequently remain androgen driven and high intratumoral androgens are often seen despite castrate levels of serum testosterone. Abiraterone acetate is a potent, selective, and orally available inhibitor of CYP17, the key enzyme in androgen and oestrogen biosynthesis.
A phase I/II study of abiraterone acetate in castrate, chemotherapy-naive CRPC patients showed a decline in PSA of > or = 50% in 28 (67%) of 42 patients, and declines of > or = 90% in eight (19%) of 42 patients. Independent radiologic evaluation with CT scans reported partial responses in nine (37·5%) of 24 patients with measurable disease. A decrease in Circulating Tumour Cell counts was also documented. The median time to PSA progression (TTPP) on abiraterone acetate alone for all phase II patients was 225 days. The addition of dexamethasone at disease progression reversed resistance in 33% of patients regardless of prior treatment with dexamethasone. Selective inhibition of CYP17 with abiraterone acetate is highly active in the treatment of CRPC.17
Preclinical and clinical studies indicate that prostate cancer growth is dependent on angiogenesis. There are two types of drugs that have shown some antiangiogenic activity in prostate cancer: COX-2 inhibitors and sunitinib.
Cyclooxygenase (COX) contributes to tumour growth by inducing newly formed blood vessels (neo-angiogenesis) that sustain tumour cell viability and growth. COX 2 inhibitors are antiangiogenic.18 A recent trial of COX 2 inhibitor celecoxib given prior to surgery for prostate cancer showed decreased tumour cell proliferation, microvessel density, angiogenesis and HIF-1 while enhancing apoptosis.19 The role of celecoxib is being evaluated in the STAMPEDE trial.20 Sunitinib is an orally administered multi-targeted tyrosine kinase inhibitor against vascular endothelial growth factor receptor (VEGFR) and platelet derived growth factor receptor (PDGFR). A phase II trial evaluated the safety and activity of single-agent sunitinib (without concurrent corticosteroids) in patients with relatively heavily pre-treated patients with metastatic CRPC that had progressed following docetaxel. There was a 12-week PFS of 75·8% accompanied by 50% and 30% PSA declines in 12·1% and 21·2% of patients, respectively, supporting sunitinib being an active agent in this disease.21
Until a few years ago after chemotherapy there were limited treatment options available to treat CRPC. With improved understanding of the biology of CRPC and the emergence of newer agents, the outlook is more encouraging. Many clinical trials are under way to test new combinations of chemotherapy agents, newer biological agents and sequencing of these agents. We hope to have newer treatments that will aim to reduce the risk of death, prevent or improve disease-related symptoms and improve quality of life for this important condition.
We have no conflict of interest
Dr Vinod Menon Mullassery, Post CCT Fellow, Mount Vernon Hospital, Rickmansworth Road, Northwood
Dr Angela Swampillai, Research Fellow University College Hospital, London, 250 Euston Road, London NW1 2PG
Dr Heather Payne Consultant Clinical Oncologist University College Hospital, London, 250 Euston Road

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...
