Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]

The European Society of Cardiology (ESC) Congress took place in Amsterdam and online between 25-28 August with over 30,000 participants. This conference report includes some of the latest clinical trial news and guidelines.

Cardiac arrest patients should be taken to the closet emergency department rather than a cardiac arrest centre, according to new research presented at the ESC Congress.
The ARREST trial investigated whether expedited transfer of out-of-hospital cardiac arrest (OHCA) patients in all hospitals in London reduced mortality compared with delivery to the closest emergency department. It found no difference in survival at 30 days in patients with resuscitated cardiac arrest in the community who were taken to geographically closest emergency department. The study also found no overall difference in neurological outcomes at discharge and at three months between groups.
In the randomised controlled trial, patients successfully resuscitated after an OHCA but without ST-elevation on their post-resuscitation electrocardiogram (ECG) were randomised pre-hospital to:
In the intervention arm, paramedics alerted the receiving cardiac arrest centre prior to arrival.
The primary endpoint was all-cause mortality at 30 days in the intention-to-treat population. Secondary endpoints included all-cause mortality at three months and neurological outcomes at discharge and three months, assessed by the modified Rankin scale and cerebral performance category (CPC) score.
Between 15 January 2018 and 1 December 2022, 862 patients were enrolled, of whom 431 (50%) were randomly assigned by London Ambulance Service paramedics to expedited transfer to a cardiac arrest centre and 431 (50%) to standard care. Some 32% of participants were women.
The primary outcome of 30-day all-cause mortality occurred in 258 (63%) of 411 patients in the cardiac arrest centre group and 258 (63%) of 412 patients in the standard care group (unadjusted risk ratio [RR] for survival 1.00, 95% confidence interval [CI] 0.90 to 1.11, p=0.96; risk difference 0.2%, 95% CI -6.5 to 6.8). There was no difference in the secondary endpoint of three-month all-cause mortality between the two groups (RR 1.02, 95% CI 0.92 to 1.12; risk difference 1.0%, 95% CI -5.6 to 7.5). Neurological outcomes were similar at hospital discharge and three months for both the modified Rankin scale (odds ratio 1.00, 95% CI 0.76 to 1.32) and CPC score (0.98, 95% CI 0.74 to 1.30).
Cardiac arrest centres provide targeted critical care, acute cardiac care, radiology services and appropriate neuroprognostication beyond what is available in conventional emergency departments. Data from non-randomised studies suggest that ambulance delivery of OHCA patients to specialist cardiac arrest centres improves survival and there is a strong drive internationally to preferentially treat cardiac arrest victims at these centres.
Study author Dr Tiffany Patterson of Guy’s and St Thomas’ NHS Foundation Trust, London, said: “This study does not support transportation of all patients to a cardiac arrest centre following resuscitated cardiac arrest within this healthcare setting. Cardiac arrest centres are heavily resourced hospitals. If delivering these patients to such centres to receive multiple interventions does not improve overall survival, then these resources are better allocated elsewhere. Furthermore, if cardiac arrest patients are not taken to such hospitals, this frees up space for other emergency work – including trauma, ST-elevation myocardial infarction and acute aortic dissection – that requires high-dependency beds and the specialist input provided by these centres.”

Semaglutide, a potent glucagon-like-peptide-1 receptor agonist, significantly improves symptoms, physical limitations and exercise function, in addition to weight loss, in patients with preserved ejection fraction (HFpEF) and obesity.
The study presented at the ESC was a randomised, double-blind, placebo-controlled trial conducted at 96 sites in 13 countries in Asia, Europe, North America and South America. The trial included patients with HFpEF (left ventricular ejection fraction ≥45%), body mass index (BMI) ≥30 kg/m2, heart failure symptoms and functional limitations (New York Heart Association functional class II–IV and Kansas City Cardiomyopathy Questionnaire Clinical Summary Score [KCCQ-CSS] <90 points).
Participants were randomly assigned in a 1:1 ratio to once-weekly subcutaneous semaglutide 2.4 mg or placebo for 52 weeks. The trial had two primary endpoints: change from baseline to week 52 in 1) KCCQ-CSS, a gold standard measure of heart failure-related symptoms and physical limitations; and 2) body weight. Confirmatory secondary endpoints included change in 6-minute walk distance (6MWD – a validated measure of exercise function); a hierarchical composite endpoint of death, heart failure events and change in KCCQ-CSS and 6MWD; and change in C-reactive protein (CRP – a measure of inflammation).
The trial included 529 patients. The median age was 69 years and 56.1% were women. The median body weight and BMI at baseline were 105.1 kg and 37.0 kg/m2, respectively. At baseline, patients had a substantial degree of heart failure-related symptoms, physical limitations and poor exercise tolerance: 66.2% were NYHA class II and 33.8% were NYHA class III–IV; the median KCCQ-CSS was 58.9 points; and the median 6MWD was 320 meters.
The trial met both primary endpoints and all confirmatory secondary endpoints. The mean change in KCCQ-CSS from baseline to week 52 was 16.6 points with semaglutide versus 8.7 points with placebo (estimated treatment difference [ETD]: 7.8 points, 95% confidence interval [CI] 4.8 to 10.9; p<0.001). The mean change in body weight from baseline to week 52 was -13.3% with semaglutide versus -2.6% with placebo (ETD: -10.7%, 95% CI -11.9% to -9.4%; p<0.001).
Principal investigator Dr Mikhail Kosiborod of Saint Luke’s Mid America Heart Institute, Kansas City, US said: “In patients with HFpEF and obesity, treatment with semaglutide 2.4 mg produced large improvements in symptoms, physical limitations and exercise function, reduced inflammation, and resulted in greater weight loss and fewer serious adverse events as compared with placebo.
“To our knowledge, this is the first trial of a pharmacologic agent to specifically target obesity as a treatment strategy for HFpEF, and the magnitude of the benefits we observed is the largest seen with any agent in HFpEF. This will likely have a significant impact on clinical practice, especially since there is a dearth of efficacious therapies in this vulnerable patient group. We believe that these findings should also change the nature of the conversation about the role of obesity in HFpEF, as the STEP-HFpEF results clearly indicate that obesity is not simply a comorbidity in patients with HFpEF but a root cause and a target for therapeutic intervention.”

A new project will examine the ability of behavioural and psychological interventions to reduce the heart damage from anti-cancer therapies for women with breast cancer.
The five-year, EU-funded CARDIOCARE project aims to radically change the management of older women with breast cancer. The project is harnessing the expertise of cardiologists, oncologists, psychologists, molecular biologists, bioinformaticians, computer scientists and biomedical engineers from seven countries across Europe to improve the monitoring, treatment and care these patients receive.
The clinical trial will evaluate the impact of behavioural and psychological interventions on quality of life, physical and mental wellbeing, and the cardiotoxic effects of breast cancer treatment in 750 patients with breast cancer at six clinical centres in Europe.
All patients in the trial will receive the CARDIOCARE mobile application (app). Participants will be randomly allocated to receive the app incorporating both ePsycHeart and eHealtHeart or to receive the app with ePsycHeart only. ePsycHeart will monitor quality of life, mobility and mental health using a wearable chest band heart rate sensor, smartwatch and questionnaires. eHealtHeart will encourage patients in the intervention group to adopt behaviours including physical activity, healthy diet, games to improve memory and changing the home environment to reduce the risk of falls.
Project coordinator Professor Dimitrios I Fotiadis of the University of Ioannina, Greece, said: “Cardiovascular disease is a devastating complication of anti-cancer treatment that affects physical and mental health. CARDIOCARE will provide women over the age of 65 with breast cancer the tools to improve their physical health and to psychologically adapt to the disease.”
Another major goal of the trial is the early identification of women with breast cancer at the greatest risk of heart and blood vessel damage from anti-cancer treatments. Cutting-edge technologies such as next generation sequencing will be used to pinpoint changes in gut microbe species that signal damage of the heart and blood vessels before symptoms occur. In addition, artificial intelligence will be used to analyse images of the heart to predict the likelihood of heart damage.
Professor Fotiadis added: “CARDIOCARE is on track to improve the physical and mental health of older women with breast cancer by detecting the cardiovascular side effects of anti-cancer treatment early and providing digital tools to help patients improve their mental and physical wellbeing.”

Immediate multivessel percutaneous coronary intervention (PCI) is non-inferior to staged multivessel PCI for reducing death and ischaemic events in patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronary artery disease, according to new results from the MULTISTARS AMI trial.
Curerent ESC guidelines state that routine revascularisation of non-infarct-related artery lesions should be considered in STEMI patients with multivessel coronary artery disease before hospital discharge. However, there is a lack of evidence on the optimal timing of multivessel PCI (immediate versus staged).
The trial investigated whether immediate complete revascularisation at the time of primary PCI was non-inferior to staged (within 19 to 45 days) multivessel PCI among haemodynamically stable patients with STEMI and multivessel coronary artery disease.
It included patients with acute STEMI (presenting within 24 hours of symptom onset) and multivessel coronary artery disease (defined as at least one coronary lesion with ≥70% diameter stenosis on coronary angiography based on visual estimation in a non-culprit coronary artery of ≥2.25 mm and ≤5.75 mm in diameter), who were haemodynamically stable after successful primary PCI of the infarct-related coronary artery.
Patients were randomly allocated in a 1:1 ratio to immediate or staged (within 19 to 45 days) PCI of the non-culprit lesions. The primary endpoint was a composite of all-cause death, non-fatal myocardial infarction, stroke, unplanned ischaemia-driven revascularisation, or hospitalisation for heart failure within one year after randomisation.
The trial enrolled 840 patients from 37 sites in Europe. The average age of participants was 65 years and 21.2% were women. At one year, the primary endpoint occurred in 35 patients (8.5%) in the immediate group and in 68 patients (16.3%) in the staged group (risk ratio 0.52; 95% confidence interval 0.38 to 0.72; p<0.001 for non-inferiority; p<0.001 for superiority). The median time interval from randomisation to staged procedures in the staged group was 37 (interquartile range 30-43) days.
Non-fatal myocardial infarction occurred in 8 patients (2.0%) in the immediate group and in 22 patients (5.3%) in the staged group (hazard ratio [HR] 0.36; 95% confidence interval [CI] 0.16 to 0.80), and unplanned ischaemia-driven revascularisation was performed in 17 patients (4.1%) in the immediate group and in 39 patients (9.3%) in the staged group (HR 0.42, 95%CI 0.24 to 0.74). Rates of all-cause death, stroke, and hospitalisation for heart failure did not differ between groups.
Principal investigator Dr. Barbara Stähli of the University Hospital Zurich, Switzerland, said: “MULTISTARS AMI addresses the clinically important question of the optimal timing for a complete revascularisation of patients with STEMI and multivessel coronary artery disease. The trial has implications for clinical practice, as it demonstrated that immediate PCI of non-culprit lesions is as effective and safe as a staged procedure. Results were generally consistent across prespecified key subgroups, particularly among women and men, young and older patients, and patients with or without diabetes.”
A study presented at the ESC found that sedentary time accumulated from childhood to young adulthood was associated with heart damage – even in those with normal weight and blood pressure.
This was the first study to investigate the cumulative effect of smartwatch-assessed sedentary time in young people and cardiac damage later in life. It was conducted as part of the Children of the 90s study, which began in 1990/1991 and is one of the world’s largest cohorts with lifestyle measurements from birth.
Study author Dr Andrew Agbaje, University of Eastern Finland, Kuopio, Finland, said: “All those hours of screen time in young people add up to a heavier heart, which we know from studies in adults raises the likelihood of heart attack and stroke. Children and teenagers need to move more to protect their long-term health.”
At 11 years of age, children wore a smartwatch with an activity tracker for seven days. This was repeated at 15 years of age and again at 24 years of age. The weight of the heart’s left ventricle was assessed by echocardiography, a type of ultrasound scan, at 17 and 24 years of age and reported in grams relative to height (g/m2.7).
The researchers analysed the association between sedentary time between 11 and 24 years of age and heart measurements between 17 and 24 years of age after adjusting for factors that could influence the relationship including age, sex, blood pressure, body fat, smoking, physical activity and socioeconomic status.
The study included 766 children, of whom 55% were girls and 45% were boys. At 11 years of age, children were sedentary for an average of 362 minutes a day, rising to 474 minutes a day in adolescence (15 years of age), and 531 minutes a day in young adulthood (24 years of age). This means that sedentary time increased by an average of 169 minutes (2.8 hours) a day between childhood and young adulthood.
Each one-minute increase in sedentary time from 11 to 24 years of age was associated with a 0.004 g/m2.7 increase in left ventricular mass between 17 to 24 years of age. When multiplied by 169 minutes of additional inactivity this equates to a 0.7 g/m2.7 daily rise – the equivalent of a 3 gram increase in left ventricular mass between echocardiography measurements at the average height gain. A previous study in adults found that a similar increase in left ventricular mass (1 g/m2.7) over a seven-year period was associated with a two-fold increased risk of heart disease, stroke, and death.
Dr Agbaje said: “Children were sedentary for more than six hours a day and this increased by nearly three hours a day by the time they reached young adulthood. Our study indicates that the accumulation of inactive time is related to heart damage regardless of body weight and blood pressure. Parents should encourage children and teenagers to move more by taking them out for a walk and limiting time spent on social media and video games.”

Patients with end-stage heart failure had lower rates of death or urgent heart transplantation with atrial fibrillation ablation compared with medical therapy, according to research presented at the ESC Congress.
The CASTLE-HTx trial enrolled patients with symptomatic atrial fibrillation and end-stage heart failure who were eligible for heart transplantation according to criteria from the ESC and the International Society for Heart and Lung Transplantation (ISHLT). Patients were in New York Heart Association (NYHA) functional class II, III, or IV, had a left ventricular ejection fraction (LVEF) of 35% or below and were fitted with a cardiac device for continuous monitoring.
Patients were randomly assigned in a 1:1 ratio to receive either first-time catheter ablation or medical therapy for atrial fibrillation (rate or rhythm control). Both groups received guideline-directed heart failure therapy. The primary endpoint was the composite of all-cause mortality, worsening heart failure requiring urgent heart transplantation, or left ventricular assist device (LVAD) implantation.
The study included 194 patients. The average age of participants was 64 years and 19% were women. The study was stopped for efficacy by the Data Safety Monitoring Board one year after randomisation was completed.
The primary endpoint occurred in 8 (8.2%) patients in the ablation group and 29 (29.9%) patients in the medical therapy group, for a hazard ratio of 0.24 (95% confidence interval 0.11 to 0.52; p<0.001).
Principal investigator Professor Christian Sohns of the Heart and Diabetes Center NRW said: “Comparing atrial fibrillation ablation with medical therapy in patients with end-stage heart failure, ablation was associated with lower rates of death, urgent heart transplantation or LVAD implantation, along with a reduction in atrial fibrillation burden and improved LVEF. Of note, listing for transplantation should not be postponed given the long waiting times and high waitlist mortality.”
New research shows that the traditional Chinese medicine qiliqiangxin reduces hospitalisation for heart failure and cardiovascular death in patients with heart failure and a reduced ejection fraction (HFrEF).
The QUEST trial evaluated the clinical efficacy and safety of qiliqiangxin on major heart failure outcomes in HFrEF patients. The trial was conducted at 133 hospitals in mainland China and Hong Kong SAR of China.
The trial enrolled adult HFrEF patients with a left ventricular ejection fraction of 40% or below and NT-proBNP of 450pg/ml or higher who had been on a stable standardised baseline treatment regimen for at least two weeks prior to enrolment. Patients were randomised in a 1:1 fashion to receive qiliqiangxin (four capsules, three times daily) or placebo on top of standard medications for chronic heart failure. The primary endpoint was a composite of rehospitalisation for worsening heart failure or cardiovascular death.
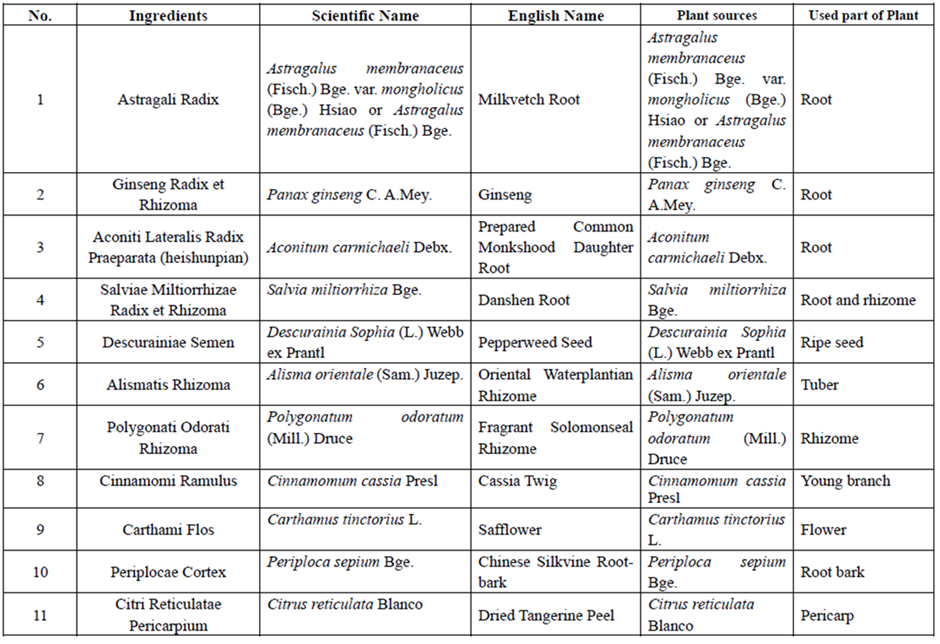
Qiliqiangxin is a traditional Chinese medicine extract obtained from 11 types of herbs (Table 1). In a pilot study, qiliqiangxin reduced N-terminal pro–B-type natriuretic peptide (NT-proBNP) levels and improved heart failure symptoms in patients with HFrEF when added to established heart failure treatment.
A total of 3,110 patients were included in the analysis, with 1,555 randomised to qiliqiangxin and 1,555 randomised to placebo. The average age was 62 years and 72.1% were men. At baseline, the mean left ventricular ejection fraction was 32%, and the median NT-proBNP was 1730.80 pg/ml.
During a median follow up of 18.3 months, the primary endpoint occurred in 389 patients (25.02%) in the qiliqiangxin group and in 467 patients (30.03%) in the placebo group (hazard ratio [HR], 0.78; 95% confidence interval [CI], 0.68 to 0.90; p<0.001). This effect was related to both lower risks of rehospitalisation for worsening heart failure (HR, 0.76; 95% CI, 0.64 to 0.90; p=0.002) and cardiovascular death (HR, 0.83; 95% CI, 0.68 to 0.996; p=0.045) in the qiliqiangxin group. The effect of qiliqiangxin on the primary outcome was generally consistent across prespecified subgroups including in the subgroups defined according to age and NT-proBNP level, and in patients with or without angiotensin receptor/neprilysin inhibitors (ARNIs).
Principal investigator Professor Xinli Li of the First Affiliated Hospital of Nanjing Medical University, Nanjing, China said: “To our knowledge, this was the first randomised, double-blind controlled trial of a traditional Chinese medicine for the treatment of chronic heart failure. Our findings demonstrate meaningful clinical benefit with qiliqiangxin in patients with HFrEF, which support the use of qiliqiangxin as an adjunct therapy for treating heart failure.”

Natriuresis guided therapy significantly increases 24-hour natriuresis in patients with acute heart failure (AHF), according to a new study.
Natriuresis is the process of sodium excretion in the urine through the action of the kidneys. Greater sodium excretion and a net negative sodium balance have been shown to be associated with better clinical outcomes for patients with AHF.
The PUSH-AHF trial therefore set out to investigate the effectiveness of natriuresis guided diuretic therapy on natriuresis and clinical outcomes in patients with acute heart failure, and to compared this to standard of care.
Standard care for AFH patients is loop diuretic therapy which helps to get rid of excess fluid. However, a large number of patients have an insufficient response to diuretics, which is associated with residual congestion and an increased risk of mortality and heart failure rehospitalisation.
In an interview with Cardiac Failure Review, principal investigator Dr Jozine ter Maaten of the University Medical Centre Groningen said: “The treatment of acute heart failure has remained unchanged for the last 50 years. We treat these patients with intravenous loop diuretics and its fascinating that at least half of these patients do not respond adequately to this only available treatment option. We also know this treatment does not result in better outcomes.”
In total, 310 patients with acute heart failure who presented at emergency departments were randomised to natriuresis guided therapy and standard of care. The study had two primary endpoints: 24-hour natriuresis, and a combined endpoint of time to all-cause mortality or heart failure rehospitalisation at 180 days.
The results revealed that natriuresis during the first 24 hours was significantly higher in the natriuresis guided versus standard of care group. While there was no meaningful difference in all-cause mortality between the two groups, there was a “remarkable difference” in in-hospital deaths between the two groups, says Dr ter Maaten.
“There were only two deaths in the natriuresis guided group compared to 14 deaths in the standard of care group. This was not, however, a prespecified outcome,” she said.
Dr ter Maaten says the results suggest that we can use urinary sodium as a personalised treatment approach for patients with acute heart failure.
“By using natriuresis guided therapy you identify patients that do not respond adequately, and we have shown that if you increase doses or administer additional doses, or even initiate combination diuretic therapy, there patients indeed pee out more sodium but they also have significantly more dieresis in the first days of hospitalisation.
“So, I think the conclusions of the PUSH-AHF is that we now have the first evidence for personalised treatment therapy in acute heart failure, and we also showed that this is safe. This therapy did not result in more electrolytes imbalances, more renal dysfunction and also did not result in adverse long-term outcomes.”

Anticoagulation after primary percutaneous coronary intervention (PPCI), also known as angioplasty or coronary angioplasty, is safe but does not reduce the risk of ischaemic events in patients with ST-segment elevation myocardial infarction (STEMI), according to new research.
PPCI is a procedure used to treat the narrowed coronary arteries of the heart and angina in patients. ESC guidelines recommend the use of intravenous anticoagulation during PPCI with unfractionated heparin, enoxaparin or bivalirudin (known as post-procedural anticoagulation, or PPA) in patients presenting with STEMI (a serious type of heart attack).
However, until now, no randomised study had looked at the risk-benefit of stopping or prolonging anticoagulation after the procedure.
The RIGHT trial therefore set out to discover whether routine use of low-dose PPA was superior to placebo after primary PCI for STEMI in contemporary practice.
The trial was conducted at 53 centres in China, and each centre chose one of three selected PPA regimens:
Patients were randomised in a 1:1 fashion to receive low-dose PPA or matching placebo for at least 48 hours. The primary objective was to demonstrate superiority of PPA to reduce the primary efficacy endpoint of all-cause death, non-fatal myocardial infarction, non-fatal stroke, definite stent thrombosis, or urgent revascularisation of any vessel within 30 days.
In total, 2,989 low-to-intermediate risk patients with STEMI undergoing primary PCI were enrolled and randomised. The primary efficacy endpoint occurred in 37 patients (2.5%) in both the PPA and placebo groups. There was no excess major bleeding globally or in any of the three anticoagulant groups
However, a significant interaction was observed for the type of anticoagulant and the primary endpoint (p=0.015):
Principal investigator Professor Shaoping Nie of Capital Medical University, Beijing, China says further studies are now needed to determine whether enoxaparin anticoagulation may be beneficial after PPCI.
Sodium glucose co-transporter-2 (SGLT2) inhibitors do not lower 28-day all-cause mortality compared with usual care or placebo in patients hospitalised with Covid-19, according to new research.
SGLT2 inhibitors are a class of prescription medicines that are used with diet and exercise to lower blood sugar in adults with type 2 diabetes.
SGLT2 inhibitors provide cardiovascular protection and prevent the progression of kidney disease in patients at risk of events such as dysregulated immune responses, endothelial damage, microvascular thrombosis, and inflammation. This treatment may also lead to organ protection in a setting of acute illness, such as Covid-19.
However, until now, the role of SGLT2 inhibitors in patients hospitalised with Covid-19 remained uncertain.
To investigate further, the World Health Organization (WHO) Rapid Evidence Appraisal for Covid-19 Therapies (REACT) Working Group conducted a prospective meta-analysis using data from randomised controlled trials evaluating SGLT2 inhibitors in patients hospitalised with Covid-19.
Three eligible trials were included, all of which compared SGLT2 inhibitors with usual care or placebo, and evaluated the impact on 28-day all-cause mortality (the primary outcome) and other efficacy endpoints in patients hospitalised with Covid-19.
Of the 6,096 participants included in the studies, 3,025 patients were randomised to SGLT2 inhibitors and 3,071 patients were randomised to usual care or placebo. There were 351 deaths in the treatment group and 382 deaths in the usual care or placebo group. This corresponded to an absolute mortality risk of 11.7% for SGLT2 inhibitors compared with an assumed mortality risk of 12.4% for usual care or placebo.
The primary safety outcome of ketoacidosis by 28 days was observed in 7 and 2 patients allocated to SGLT2 inhibitors and usual care or placebo, respectively. Overall, the incidence of reported serious adverse events was balanced between treatment groups.
Presenting author Dr. Mikhail Kosiborod of Saint Luke’s Mid America Heart Institute, Kansas City, US said his team found “no convincing evidence” that of SGLT2 inhibitors reduce 28-day all-cause mortality or improve other pre-specified efficacy outcomes.
“These findings do not support the use of SGLT2 inhibitors as standard care in this clinical setting. No new safety signals were observed with the use of SGLT2 inhibitors in this patient population, and their routine discontinuation during acute illness for patients that receive them for other indications such as heart failure, chronic kidney disease, or type 2 diabetes does not appear to be warranted,” he said.

Inorganic nitrate reduces contrast-induced nephropathy (CIN) – a complication that results in the impairment of kidney function – compared to placebo in patients at risk of renal injury undergoing coronary angiography for acute coronary syndrome.
CIN is a serious complication of coronary angiography, a procedure that uses a special dye (contrast material) and x-rays to see how blood flows through the arteries in the heart.
Older age, heart failure, chronic kidney disease and diabetes are independent predictors of CIN following coronary angiography for acute coronary syndromes, and CIN is associated with longer hospital stays, an increased risk of myocardial infarction and higher mortality.
Inorganic nitrate is metabolised in the body to deliver nitric oxide to areas of the body in need and has shown renoprotective effects in preclinical studies. The NITRATE-CIN trial therefore set out to examine the efficacy of inorganic nitrate for the prevention of CIN in patients with non-ST elevation acute coronary syndrome referred for invasive coronary angiography and at risk of CIN.
In total, 640 patients were randomised at a 1:1 ratio to receive inorganic nitrate or placebo. Just under half (45.9%) had diabetes, and 56.0% had chronic kidney disease. The median follow up was 1 one year.
The primary endpoint was the incidence of CIN as defined by the Kidney Disease Improving Global Outcomes (KDIGO) criteria for acute kidney injury. Secondary outcomes included renal function (eGFR) at 3 months, rates of procedural myocardial infarction and major adverse cardiac events at 12 months.
Inorganic nitrate treatment significantly reduced CIN rates (9.1%) versus placebo (30.5%). This difference persisted after adjustment for baseline creatinine concentration and diabetes status. Secondary outcomes were improved with inorganic nitrate, with lower rates of procedural myocardial infarction (2.7% vs. 12.5%), improved 3-month renal function and reduced 1-year MACE (9.1%) versus placebo (18.1%).
Study author Dr. Dan Jones said: “These findings could have important implications for health systems by reducing the burden of CIN and the associated prolonged admissions, dialysis, and significant costs. Further studies powered for adverse cardiac events are needed to confirm these findings.”

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...