Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]

Parkinson’s disease (PD) is a neurodegenerative disorder caused by a deficiency in dopamine, normally produced by neurons in the substantia nigra of the brainstem. It is commonly seen in the older patient with an overall prevalence of ~160 per 100, 000 in the general population1 and presents with tremor, bradykinesia, and limb rigidity, as well as gait and balance problems.2
Although the underlying causes are not fully understood, there have been many successful advances in the management of Parkinson’s disease. Patients with this condition are also known to have multiple associated health problems such as delirium, adverse drug reactions, syncope, falls and fractures.3 In particular, mental health can be a significant burden of Parkinson’s that can be secondary to the condition itself and can even further impair prognosis of these patients.
Neuropsychiatric symptoms of Parkinson’s disease include depression, anxiety, apathy and psychosis.4,5 One study showed the factor most closely associated with quality of life in patients with Parkinson’s disease was the presence of depression (as well as disability, postural instability and cognitive impairment).6
Depression affects between 30-40% of PD patients, but as few as 20% of patients receive treatment for this.7 Similarly, anxiety symptoms, affecting up to 40% of patients,8,9 are also poorly attended to by clinicians despite their association in exacerbating motor symptoms.7 This highlights the need for more input and larger emphasis placed on mental health in these patients to help improve outcomes.
Mental health issues in Parkinson’ disease have been well recognised for many years. Patients with any long-term comorbidities (including Parkinson’s disease) commonly experience mental health problems.10 As a result of these further complications due to mental health, the cost of care has increased by an average of 45%.11 On the other hand, providing treatment can save approximately £1, 760 in annual expenditure in healthcare costs12 across all patients. Given these figures, it is difficult to understand why more resources are not utilised to target this group. This article aims to discuss common mental health issues (depression and anxiety) in Parkinson’s disease patients, methods for identifying them and the current evidence for how they can be better managed.
Effective diagnosis of depression remains challenging for numerous reasons. The main subtypes of depressive diagnoses in PD (major depression, minor depression and dysthymia) are similar to those of depressive subtypes in non-PD populations.13 The main obstacle is the overlap between major depression and Parkinson’s disease itself (Table 1), therefore differentiation can be problematic.13
The key characteristics of depression are low mood and anhedonia, with other symptoms occurring in varying combinations e.g. weight loss, lethargy, reduced memory, altered sleep.14 This is seen especially in later stages of Parkinson’s’ disease, where slowness of movement and thinking, loss of appetite and sleep disorders can be manifestations of progressive PD and are comparable to somatic symptoms of depression.14
Furthermore, PD-specific features (e.g. medication side effects, having an incurable progressive disease and increased occurrence of other psychiatric comorbidities such as impulse control disorders/psychosis) can complicate the assessment for a depressive disturbance.13 In addition, direct inquiry about mood symptoms is vital for detection of depressive disturbances13 – in patients with cognitive decline this also poses a further problem.
|
Major depression |
Parkinson’s disease |
|
|
Motor phenomena |
Psychomotor retardation, stooped posture, restricted/depressed affect, agitation
|
Bradykinesia, stooped posture, masked face/hypomimia, tremor |
|
Other somatic complaints |
Physical complaints, muscle tension, GI symptoms, sexual dysfunction
|
|
|
Vegetative changes |
Decreased energy, fatigue, sleep and appetite changes.
|
|
|
Cognitive disturbances |
Poor concentration, decreased memory, impaired problem-solving |
|
Table 1. Overlapping clinical features of major depression and Parkinson’s disease13
The gold standard method of diagnosis of depression in PD is based on clinical interview and fulfilling criterion based on DSM IV criteria. This is despite the criteria excluding depression in those with a background of conditions such as PD.15 There are various scales used to assess depression in PD (table 2), however again these questionnaires do not address the overlap in symptoms. In addition, it is important to also highlight the inconstant psychometric properties of these scales when used on patients with PD.15 A revised DSM IV has recently been proposed by an NINDS/NIMH working group with recommendations on how to apply the DSM IV in patients with PD.
These recommendations include using all symptoms irrespective of potential aetiological bases (as opposed to not disregarding symptoms by attributing them solely to PD), as well as specifying timing of the assessment in regard to “on” vs “off” periods of PD where symptoms may be variable. In addition, they suggest using informants for patients who are cognitively impaired to overcome difficulties with patients who cannot self-report symptoms.
Furthermore, they also recommend diagnosis of anhedonia to be based on patient’s loss of pleasure rather than interest (to prevent overlap with apathy, which can present independently) to enable diagnosis of subsyndromal depression (minor depression).14,16
Following these recommendations may enable greater recognition of patients with PD suffering with depression. It is also significant in allowing us to identify and work with these patients to enhance our understanding and increase research opportunities.
|
Syndrome |
Subtype |
Prevalence |
Key features |
Diagnostic criteria in PD |
Rating scale |
|
Depression |
Major depression |
10-30% |
Low mood or loss of interest/pleasure |
NINDS-NIMH |
BDI, Ham-D, HADS, SDS, GDS, MADRS, UPDR Part I, CSDD, CES-D, depending on purpose. |
|
Minor depression |
10-20% |
Low mood and/or loss of pleasure Low mood and/or loss of pleasure Low mood and/or loss of pleasure Low mood or loss of interest/pleasure |
NINDS-NIMH |
Not validated |
|
|
Dysthymia |
10-20% |
Low mood > 2 years |
NINDS-NIMH |
Not validated |
|
|
Total |
30-40% |
None |
BAI, HADS, SAS, ASL, STAI, HARS, item five of the NPI. |
Table 2- summary of subtypes, their prevalence, features, diagnostic criteria, rating scales available for depression Parkinson’s14
The most common anxiety disorders found in Parkinson’s disease are panic disorder, generalised anxiety disorder and social phobia, however other phobias and obsessive-compulsive disorder are also notable in PD patients.17 In a subgroup of patients, anxiety also presents as a ‘reactive response’ secondary to the psychological and physical stress of the chronic disease.18
Again, there may be overlaps between symptoms of depression and anxiety, however features of anxiety that help distinguish it are the presence of apprehension, fear and worry.19 As with diagnosis of depression, difficulties arise when clinically significant presentations of anxiety in PD patients do not meet the DSM -IV criteria which require 6 months of prominent tension, worry or apprehension, alongside the presence of three of six other symptoms. Unfortunately, these additional symptoms include sleep disturbance, difficulty concentrating and muscle tension which may all be attributed to by Parkinson’s disease itself.20
The three most commonly used scales for diagnosing Anxiety are the Beck Anxiety Inventory (BAI), the Hospital Anxiety and Depression scale (HADS) and Hamilton Anxiety Rating Scale (HARS), which have all been validated for use in PD.21 These scales, however, are aimed at the general population and were not designed to meet needs and challenges of patients with Parkinson’s disease. The Parkinson Anxiety Scale (PAS) has been developed to target Parkinson’s disease patients and is reported to have a greater specificity and sensitivity than other existing scales.22
In addition, the Geriatric Anxiety Inventory (GAI) has also been developed for PD patients but requires further studies to understand it’s efficacy.21
Recently updated NICE Parkinson’s guidelines23 does not address or provide specific recommendations for mental health problems in these patients,12 instead referring to the existing generic guidelines on depression in adults with a chronic health problem. This is a failing when compared to other neurological conditions such as multiple sclerosis, which have guidelines including recommendations for regular screening for cognitive, emotional or mental health problems.12
There are various barriers in mental health care management in PD. Commonly, these barriers reflect patients being unable to completely understanding their mental health problems, struggling to access health care and illness-specific concerns. In addition, inadequate screening and detection by carers and the need for more effective treatments.24 With the aid of recommendations discussed above, some obstacles have greater potential to be overcome. For example, the with the clarification of “on” and “off” periods we can exclude patients having symptoms of “off” periods overlapping with potential depressive features, who may just need optimisation of levodopa medication.14
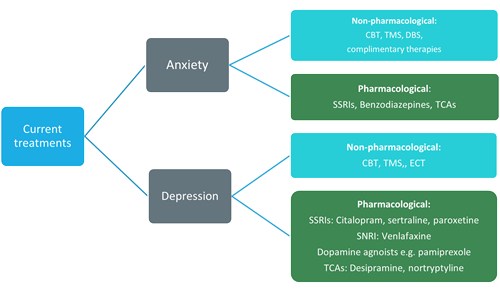
Figure 1. Summary of current treatment options for depression and anxiety in Parkinson’s disease
There is also good evidence for the use of cognitive behaviour therapy (CBT) showing evidence of improved mood for up to 6 months. However there is still little evidence for the long-term benefits of CBT.21 There is a some evidence suggesting transcranial magnetic stimulation has a beneficial effect on mood symptoms, whereas deep brain stimulation has been associated with worsening mood, including the increased risk of suicide following surgery.21Unfortunately, currently there is a lack of evidence for safety as well as efficacy of treatment options in Parkinson’s patients. Non-pharmacological interventions as part of an MDT approach, including education about mood disturbances in Parkinson’s disease and how to cope with/manage such symptoms, are effective as initial management of depression.21
Current studies for the pharmacological management of depression shows effective treatment with the use of specific tricyclic antidepressants (Desipramine and Nortriptyline), serotonin reuptake inhibitors (SSRIs) (Citalopram, Sertraline and Paroxetine), and Venlafaxine (serotonin-noradrenaline reuptake inhibitor, SNRI). In addition to this, dopamine agonists, such as Pramipexole and Rotigotine, have also been found to exert antidepressant properties.21
Meanwhile, there much less evidence for treatment options for Anxiety. Non-pharmacological treatment involves various therapies including CBT and transcranial magnetic stimulation (TMS) as with depression. Deep brain stimulation (DBS) has been found to particularly useful in improving motor symptoms and improving quality of life, therefore reducing the risk of inducing anxiety. However as mentioned earlier DBS poses other risks (i.e. suicidal attributes). Multiple complimentary therapies have also been studied and found to be effective, in particular when struggling with the complications of pharmacological treatments. These include Ayurveda, meditation, yoga, music therapy and aromatherapy.18
Of the numerous anxiolytic agents available, benzodiazepines, TCAs and SSRIs/SNRI (e.g. citalopram, sertraline, venlafaxine) have been evaluated for use in Anxiety, despite primarily made to target depression. In particular, the use of higher doses of SSRIs/SNRIs have been associated with greater likelihood of treatment response. Unfortunately, they also come with side effects including agitation, sexual dysfunction, worsening sedation, nausea, and endocrinological and metabolic adverse effects, thus may not be tolerated. Benzodiazepines are almost as effective and produce fewer side effects of ataxia and sedation.
However, usage on an as-required regime means dependence is very likely resulting in reinforcement of avoidance and long-term reliance on the medication. For this reason, SSRIs are still used first line if tolerated. In addition, benzodiazepines with shorter half-lives (e.g. alprazolam, lorazepam) are preferred to reduce accumulation and risk of side effects.19 Other medications are also available such as TCAs (nortriptyline, amitriptyline)25 have similar efficacy to SSRIs when used for panic attacks or GAD, however, have a worse side effect profile including dry mouth, headache, blurred vision, constipation and urinary retention.18
|
Class of drug |
Specific drugs |
|
|
Depression
|
Selective serotonin reuptake inhibitors |
Citalopram Sertraline Paroxetine |
|
Serotonin-noradrenaline reuptake inhibitors |
Venlafaxine |
|
|
Dopamine Agonists |
Pramipexole Rotigotine |
|
|
Tricyclic antidepressants |
Nortriptyline Desipramine |
|
|
Anxiety |
Selective serotonin reuptake inhibitors Serotonin-noradrenaline reuptake inhibitors |
Citalopram Sertraline Venlafaxine |
|
Benzodiazepines |
Alprazolam Lorazepam |
|
|
Tricyclic antidepressants |
Nortriptyline Amitriptyline |
Table 3. Summary of pharmacological management in depression and anxiety
Mental health in Parkinson’s disease is still greatly misunderstood due to the lack of research dedicated to it. Given the implications of mental health on the trajectory of the disease and the high likelihood of developing such problems, as well as the great burden it adds to these patients, more needs to be done to attend to them.
The Parkinson’s Mental Health Enquiry conducted in May 2018 as well as the ‘Five Year Forward plan’ alongside this are steps in the right direction, highlighting current failings with aims to address them in the future. However, one of the main barriers we face is the lack of research on how to manage these comorbidities. Despite this, there are still interventions available but this requires clinicians to spend time on identifying those who may be suffering with Depression or anxiety, and using the tools and treatments currently available. Simple methods, such as increasing screening and using better tools for identification, are changes which physicians can make in daily practice that can themselves greatly aid these patients.
There is a potential to make a huge difference to the outcomes of these patients and significantly improve the quality of their lives, their prognosis, the impact on their families and those involved in their care.
Dr Sanggeeta Surandran, junior doctor, Colchester hospital,
Dr Nadeem Aftab, Geriatrician at Colchester Hospital
*Beck Depression Inventory (BDI), The Hamilton Depression (Ham-D) Rating Scale, The Hospital Anxiety and Depression Scale (HADS), the Geriatric Depression Scale (GDS), the Montgomery–Asberg Depression Rating Scale (MADRS), the Unified Parkinson’s Disease Rating Scale (UPDRS), Cornell Scale for the assessment of Depression in Dementia (CSDD), Centre for Epidemiologic Studies Depression scale (CES-D), Beck Anxiety inventory (BAI), the Zung Self-rating Depression Scale (SAS), Anxiety Status Inventory (ASI), Speilberger State Trait Anxiety Inventory (STAI), Hamilton Anxiety Rating Scale (HARS), Neuropsychiatric inventory (NPI); NPI, neuropsychiatric inventory; SSRI, selective serotonin reuptake inhibitors; SSNRI, serotonin and noradrenaline re-uptake inhibitor; SNRI, selective noradrenaline re-uptake inhibitor.

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...