Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]

Psoriatic arthritis is an inflammatory arthritis that is associated with psoriasis. Published estimates of psoriatic arthritis incidence vary widely, but it is accepted that around one in five people with psoriasis develop psoriatic arthritis.1,2 Although there is a school of thought that those with severe psoriasis are the most at risk, in practice joint disease does not always correlate with the skin.3 Most people will have psoriasis first, but a certain number will present to their GP with joint issues that have no history of psoriasis. Anecdotally, we hear that some of these people may have skin involvement so mild or hidden they may not have noticed or had it diagnosed.
Psoriatic arthritis can cause irreversible joint damage if not treated effectively early on, which may result in loss of function and long-term disability.4 It is therefore crucial to recognise the signs of psoriatic arthritis early. Diagnosis can be difficult as there is no one definitive sign or test, and many of the signs and symptoms are similar to other conditions. Anecdotally at the Psoriasis Association, we commonly hear of psoriatic arthritis being misdiagnosed as tendonitis, ‘wear and tear’, gout, other types of arthritis (such as rheumatoid), and fungal nail infections. Common signs and symptoms of psoriatic arthritis include:
Psoriatic arthritis can occur in any area in the body where tendon joins to bone, including the lower back, neck, pelvis, elbow, and weight-bearing joints such as the knee and heel. There are numerous patterns of presentation. It is particularly common in the small joints of the hands and feet, and so people with psoriasis presenting with hand, foot and digit issues need to be considered for the possibility of psoriatic arthritis.
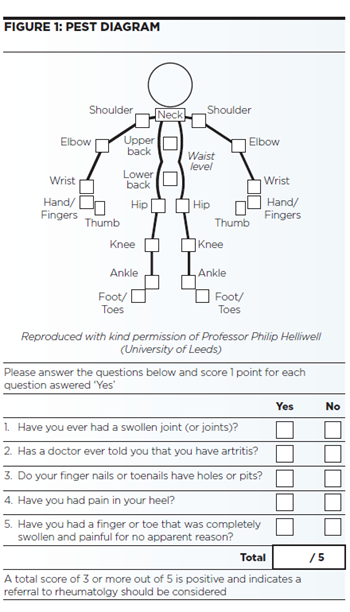
At present, there is no diagnostic criteria that is sensitive enough to diagnose psoriatic arthritis in non-specialist settings. NICE recommends that every person with psoriasis is offered an annual assessment for psoriatic arthritis. It recommends using a validated screening tool to do this, particularly the Psoriasis Epidemiological Screening Tool (PEST), which asks the patient five closed questions about the existence of joint swelling, nail changes, dactylitis and other key signs, as well as to indicate the joints they have suffered discomfort in on a stick man figure.
A score of three or above indicates that a referral to rheumatology should be considered. Psoriatic arthritis is distinct from rheumatoid arthritis, and a test for rheumatoid factor will be negative in many cases. It is crucial to use this test to rule out the possibility of rheumatoid arthritis only – not inflammatory arthritis altogether. NICE guidance on spondyloarthritis in over 16s (NG65) advises not to rule out a diagnosis based on any single sign, symptom or test result.
The same guidance also advises that, in specialist settings, x-ray and MRI imaging may be used to check for tell-tale changes including erosions and ossifications8 (new bone growth within the joint).
Without effective treatment, psoriatic arthritis can cause irreversible damage, loss of function and long-term disability. GPs are therefore perfectly placed to spot signs of the disease promptly, allowing for early referral and effective treatment, and therefore the best possible outcome for the patient.
NICE recommends that as soon as psoriatic arthritis is suspected – ideally using the PEST tool (see Figure 1), the patient should be referred to a rheumatologist, who can confirm what can be a difficult diagnosis, and administer disease-modifying treatment to help prevent the arthritis progressing and causing irreversible damage. There are numerous treatment options for people with psoriatic arthritis, but an important distinction needs to be made between treatment that eases symptoms, and treatment that is ‘disease modifying’, and therefore stops the arthritis from progressing.
In primary care, non-steroidal anti-inflammatory drugs are available which can improve pain and swelling, and therefore make the patient more comfortable and may improve their ability to go about day-to-day life. Similarly, in secondary care, a rheumatologist may choose to use a corticosteroid injection into a singular joint to reduce inflammation and improve pain and joint utility. These drugs will have no effect on the underlying disease, but are often useful as part of a wider treatment plan.
Disease-modifying anti-rheumatic drugs (DMARDs) are immunosuppressive drugs that are commonly used in psoriatic and other types of arthritis, with the aim of reducing the inflammatory activity in the immune system that causes the arthritis. The traditional systemic DMARDs commonly used in psoriatic arthritis include methotrexate, leflunomide, sulfasalazine (the exact mode of action in psoriatic arthritis for each of these agents is unknown, but they are established immunosuppressives commonly used in other types of inflammatory conditions) and, more recently, apremilast (which inhibits the enzyme phosphodiesterase 4 and inhibits spontaneous production of TNF- alpha, which is thought to be involved in the inflammatory processes associated with psoriatic arthritis).
Tofacitinib is a Janus Kinase (JAK) inhibitor. It works differently to any of the other treatments that are currently available to treat psoriatic arthritis. Tofacitinib stops the activity of JAK enzymes, meaning that the inflammatory cycle of psoriatic arthritis is disrupted. Tofacitinib is a tablet that is taken twice a day. At the moment, it can only be prescribed to people who have tried other DMARDs, including certain biologic treatments, and found that these have not worked or have stopped working.
These should be initiated under the supervision of a rheumatology specialist, but the collaboration of primary care colleagues is essential in the regular monitoring that most DMARDs require.
Depending on the specific treatment used, there should be regular monitoring for possible systemic effects such as leucopenia and hepatic toxicity, amongst others. This is usually arranged via Shared Care Agreements, and advised frequency differs depending on which treatment is being used, but usually monitoring will be carried out more frequently (i.e., fortnightly or monthly) during the first six months of treatment, until the patient is considered stable. Thereafter, monitoring may be reduced in frequency dependent on clinical judgement and discussion with the specialist team.
Similarly, due to their immunosuppressive nature, infections are common and patients are advised to have an annual influenza vaccination. The recently-licensed apremilast does not have the same possible effects, and thus does not require regular monitoring.
There are numerous biologic drugs that are licensed and recommended for use in people with active psoriatic arthritis (defined as three or more tender joints, and three or more swollen joints), who have used at least two conventional DMARDs without lasting success.10 It is recommended that an anti-TNF drug is used first, followed either by alternative anti- TNFs, or the more-recently licensed interleukin drugs.
NICE published a Covid-19 rapid guideline on dermatological conditions treated with drugs affecting the immune response. The purpose of this guideline is to maximise the safety of children and adults who have dermatological conditions treated with drugs affecting the immune response during the Covid-19 pandemic. It also aims to protect staff from infection and enable services to make the best use of NHS resources.
It is believed that the Pfizer/BioNTech, Oxford/AstraZeneca and Moderna vaccines are all considered suitable for people who are living with psoriasis and/or psoriatic arthritis regardless of whether they are receiving drugs that affect the immune system (such as methotrexate and biologic injections, for example) or not.
Information and support can be major factors in helping a person with psoriatic arthritis to cope effectively with their condition. Many people feel alone and isolated, and, unfortunately, the internet and mainstream media is full of inaccurate information on the condition.
The Psoriasis Association offers good quality, Information Standard-accredited information free of charge through its website and telephone and email helpline (01604 251620/[email protected]). Additionally, the Psoriasis Association also manages online communities via a website forum and social media, as many people find it beneficial to be able to talk to others with the condition about their experiences.
Carla Renton, Information and Communications Manager, Psoriasis Association
* Article first published on our sister publication British Journal of Family Medicine in 2018. Updated with new guidance in February 2021

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...