Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]

Alcohol misuse in older individuals is common but can be missed both in primary and secondary care. In this recent interactive webinar, sponsored by Grunenthal Meds, we asked four healthcare professionals to review a case study and discuss the multidisciplinary approach to uncovering and managing high-risk alcohol use.
The case study
A 75-year-old woman is seen in the emergency room after an unwitnessed fall. She reports she stumbled and lost her balance on the way to the bathroom. She is aware she has hurt her ankle and wrist and recalls hitting the ground. She was able to reach the phone in her bedroom and call for help.
There are no preceding symptoms of chest pain, palpitations, breathlessness, or dizziness. She has no visual or hearing impairment. There is no known neurological disease, but her son reports some forgetfulness and erratic behaviour. There is some muscle wasting but she does not use a walking aid. She has had one previous fall but has no fear of falling.
Presentation:
The patient has hypertension and atrial fibrillation. She is currently on seven medications: amlodipine, furosemide, simvastatin, apixaban, alendronate, calcium, and vitamin D.
She is a current smoker with a 20-pack year history. She reports having some whiskey each night to help her sleep and wine with dinner.
The patient lives alone following the death of her husband two years earlier. He had dementia and she had been his carer for over eight years. She has two children – both of whom live away from her.
 Dr Elena Mucci, Consultant Physician and Geriatrician, East Sussex Healthcare Trust
Dr Elena Mucci, Consultant Physician and Geriatrician, East Sussex Healthcare Trust
As a geriatrician, when you look at this case study, what are your immediate red flags?
From a doctor’s perspective, there are a lot of red flags in this case study, but we need more of a social history to understand what is going on here.
This is a classic scenario that I see every day either on the ward or in the emergency department. With a patient like this, a good starting point is to discuss the exact number of units of alcohol she consumes during a week. Current government guidance advises that men and women do not to drink more than 14 units a week on a regular basis[1]. But this is problematic as the guidance is the same for a healthy 30-year-old man as it is for a 75-year-old woman with various comorbidities.
The Royal College of Psychiatrists has recommended that older people should drink no more than 11 units of alcohol each week[2], however, I think this should be lower still at seven units.
This is because as you get older, your liver is much slower at metabolising alcohol, and it can stay in your blood stream for longer. This means that the previous day’s alcohol could still be circulating in your blood putting you in a constant state of hangover. This can lead to tiredness, drowsiness, recurrent falls, and cognitive impairment[3].
Even if we assume from the case report that she drinks one whiskey and one glass of wine at most, this would be a minimum of four units a day, which equals 28 units a week – well above the government recommendation for alcohol. This is a modest estimation as her intake could be a lot more[1].
What are the health consequences of alcohol misuse?
The immediate diagnosis that comes to mind when an older patient presents after a fall is a urinary tract infection. High-risk alcohol use would usually be low on the list of differentials, especially as there are so many other pressing issues that could cause falls. I also think there is an element of respect for elders that makes us not quiz them enough on their alcohol intake.
Cognitive impairment is a huge issue and is certainly a red flag for the lady in our case study. This could be a contributing factor to her falls – not necessarily from being intoxicated at the time, but by the chronic effect of alcohol over many months or years. These effects include drowsiness, muscle weakness and proximal myopathy. All of these are problems I see in my clinics.
What steps would you take to assess the patient’s memory function?
A screening tool that is effective in the emergency department or in a busy clinic is the Abbreviated Mental Test Score (AMTS) – a 10-question test which can be administered within two minutes[4]. The clock drawing test is also useful to check the executive function of the brain. This is the part of the brain that is responsible for planning, processing and many other functions that are needed for day-to-day living[5].
The patient in the case study would also require a comprehensive geriatric assessment. Alcohol is a diuretic[6] and she’s already on frusemide, so it is no wonder she is dehydrated. Her blood pressure appears to be on the higher side too, but how do we know if it is a stress response to being in the emergency department? We would need to do a lying to standing blood pressure assessment to see whether there are postural symptoms that are a contributing cause of her fall.
Every year, at least two or three people in my clinic are cured of dementia by ceasing alcohol use. In these types of patients, if they do present with cognitive impairment then I will try to get them to stop drinking alcohol completely. You need to show them what the future will look like if they stop drinking alcohol: their memory will get better and some do manage to get their life back. It is such a big reward.
 Dr Michael Jackson, Lead Pharmacist for Cardiothoracic Services, East Kent Hospitals University Foundation Trust
Dr Michael Jackson, Lead Pharmacist for Cardiothoracic Services, East Kent Hospitals University Foundation Trust
As a pharmacist, when you look at this case study, what are your immediate red flags?
During the Covid-19 pandemic, we saw an increase in alcohol use in our older population mostly due to social isolation. We have also seen an increase in cardiovascular disease (CVD) related incidents, such as arrhythmia management, and some of this is related to alcohol use.
One of the roles that pharmacists and pharmacy technicians undertake is medicines reconciliation, which is the process of curating and compiling an accurate and up- to-date list of medications. This is an opportunity to ask specific questions about a patient’s alcohol intake.
I want to look specifically at the consequences of alcohol use on the patient in terms of cardiovascular management. Clearly, her blood pressure is high, but there are other red flags like her weight and forgetfulness. We also need to think about the consequences of alcohol on the patient’s immediate medicines and whether they are affecting her ability to comply and adhere to medicines.
What impact can alcohol misuse have on certain medications?
Higher alcohol use can increase your risk of hypertension and coronary heart disease 1.4-fold, hence why we use alcohol intake as part of our CVD assessment[7].
We often have a stereotypical person in mind when we think of high alcohol use. You may not want to ask probing questions to the lovely older lady sitting in front of you, but one of the skills that we have as healthcare professionals is knowing how to get the right information out of our patients.
What do we know from the case study? We know she has hypertension and atrial fibrillation, but what effect does this have? Alcohol can increase blood pressure as it affects the body’s baroreceptor responsiveness. It can also hinder the body’s ability to gain blood pressure whenever you stand up very quickly, so this patient’s risk of having some sort of postural drop is very high. That standing and sitting blood pressure reading is therefore very important.
However, what we shouldn’t be doing in the hospital setting is amending a patient’s blood pressure medication unless there is a need to deprescribe. This is because if you increase it, the patient may have problems once they leave the hospital because, as Dr Mucci stated, it could be a stress response to being in hospital.
How should the role of pharmacists be broadened to include alcohol awareness and advice on medicines?
In terms of CVD risk prevention, it is important to advise a patient with hypertension to cut down on alcohol intake slowly and then abstain to bring their blood pressure down.
In addition to this, we should be aware of interactions between alcohol and certain medicines in the emergency department, which can cause things like flushing, sweating, nausea, and vomiting.
From a pain point of view after a fall, the use of IV paracetamol is very prevalent but we need to be very careful that we consider the patient’s alcohol intake because it can affect the dose of paracetamol we give. Patients with high alcohol use may also have more side effects from pain killers, such as drowsiness.
There is also a risk of overdose, especially with antihistamines, hypnotics, and opiates, and we need to be very mindful of this.
 Kate Pronger, Lead Alcohol Liaison Nurse, Aneurin Bevan University Health Board
Kate Pronger, Lead Alcohol Liaison Nurse, Aneurin Bevan University Health Board
As an alcohol liaison nurse, when you look at this case study, what are your immediate red flags?
An immediate red flag for us would be the fact that she is 75 years old. In the UK, daily alcohol consumption is growing in this age group and there has been a huge increase in the number of women drinking alcohol in later life.
This patient has been admitted with a fall, but intoxication isn’t always the cause. It could be a result of neurological changes and one of the symptoms could be an unsteady gait, so I would be thinking about what is possibly causing that.
She reports drinking whiskey each night to sleep and wine with dinner which indicates some sort of alcohol dependence, so clarifying the strength and the volume consumed is very important. Questions we should ask the patient include: what time is that first glass of wine and how big is that glass; do you finish that bottle once it is open; what sort of whiskey are you drinking; who buys it for you and how much do you spend each week?
We all know that patients often underreport their drinking behaviours, so it is very important to know exactly what we are dealing with. This means we can preempt any issues further down the line with alcohol withdrawal.
As people get older, losses, life changes, and transitions associated with ageing can result in isolation, particularly since the pandemic, I’ve spoken to numerous people, not just older patients, that have experienced isolation and a massive increase in their alcohol intake since the pandemic. For older patients, loss of independence, loneliness and psychological distress can all be contributors to starting or escalating alcohol use in later life.
The lady in our case study lives alone so she is isolated. When we think about older adults, they have fewer social roles, so their alcohol misuse is more likely to go unnoticed. A younger person might be attending work and regularly meeting with friends, and people may notice that they are disheveled, or they might smell alcohol on them. This is less likely for socially isolated older adults.
We also need to gather as much social history as possible to get a timeframe which will allow us to formulate a management and support plan.
What additional assessments would you undertake?
As a prescriber, I can make sure that the correct medication is prescribed to manage possible withdrawal symptoms to avoid future complications.
Other assessments I would undertake would be a gait assessment, as an unsteady, staggering shuffle could be associated with cerebellar ataxia, consistent with alcohol-related brain damage[8]. The lady in our case study is also malnourished, so all these symptoms would give us a high suspicion of possible Wernicke’s encephalopathy.
I would also carry out a capacity assessment to determine if this lady is able to make decisions about stopping drinking, and whether intervention or referral from other services will be required. It is also important in this patient group to check their understanding of conversations about their drinking.
I would also look back at her admission history because alcohol-related admissions can present with many different things, such as falls, daytime drowsiness, anxiety, new difficulties in decision-making, self-neglect and weight loss.
We know from looking at alcohol-related deaths, that there’s an average of five missed opportunities for services to be involved with the patient in hospital admissions alone. Regardless of whether the patient is 30 or 80, we need to be asking questions around alcohol use, especially as we know this generation might not be as forthcoming with the information due to the shame and generational differences in pride. As clinicians, I think we can be guilty of focusing on physical health issues rather than looking at whether social issues could be contributing to health issues.
What role do alcohol care teams play in helping patients recognise and reduce unhealthy drinking behaviours?
In our hospital we have excellent relationships with the wider multidisciplinary team, especially our pharmacists. We get a lot of referrals from the pharmacy team, which allows us to capture high-risk patients. Our role is to make sure the patient has a clear picture of the impact alcohol is having on their health and build the foundations for their recovery. We can then link them with our recovery teams in the community.
There is a mistaken belief that long-term habits in older adults cannot be changed, but they have been proven to be more likely to stick with treatment and have good outcomes. For example, our team recently started supporting an 84-year-old gentleman who was admitted six months ago following a fall. It transpired that he had lost two children in separate incidents and had been binge drinking to manage the trauma. He is now doing exceptionally well with the right support. His wife told us that she’s very aware there is more time behind them than what’s ahead of them, but she feels like she’s got her husband back, and she knows their remaining time isn’t going to be miserable anymore.
My takeaway message is that regardless of a person’s age, alcohol teams need to be in contact with high-risk patients at the earliest opportunity. This will result in shorter durations of treatment, less reliance on ambulance services, and lower rates of hospital admissions.
 Rhian Booth, Gastroenterology Specialist Dietitian, Wales
Rhian Booth, Gastroenterology Specialist Dietitian, Wales
As a dietitian, when you look at this case study what are your immediate red flags?
As a dietician, I’m looking at red flags such as muscle wasting, dehydration, weight loss, and low BMI. This is in addition to things like low haemoglobin and potassium. In this case study, it is clear the patient has malnutrition, which can lead to sarcopenia and micronutrient deficiencies.
It is not uncommon to find malnutrition in older patients. In the UK, one in 10 people over the age of 65 are malnourished or at risk of malnutrition, which is about 1.3 million people[9].
How would you identify the risk factors for malnutrition?
There are many risk factors for malnutrition (see Figure 1). In this case, the patient’s smoking and alcohol history and potential social isolation are clear risk factors. I also often hear from my patients that they lose the drive to cook for themselves following the death of a partner or loved one.
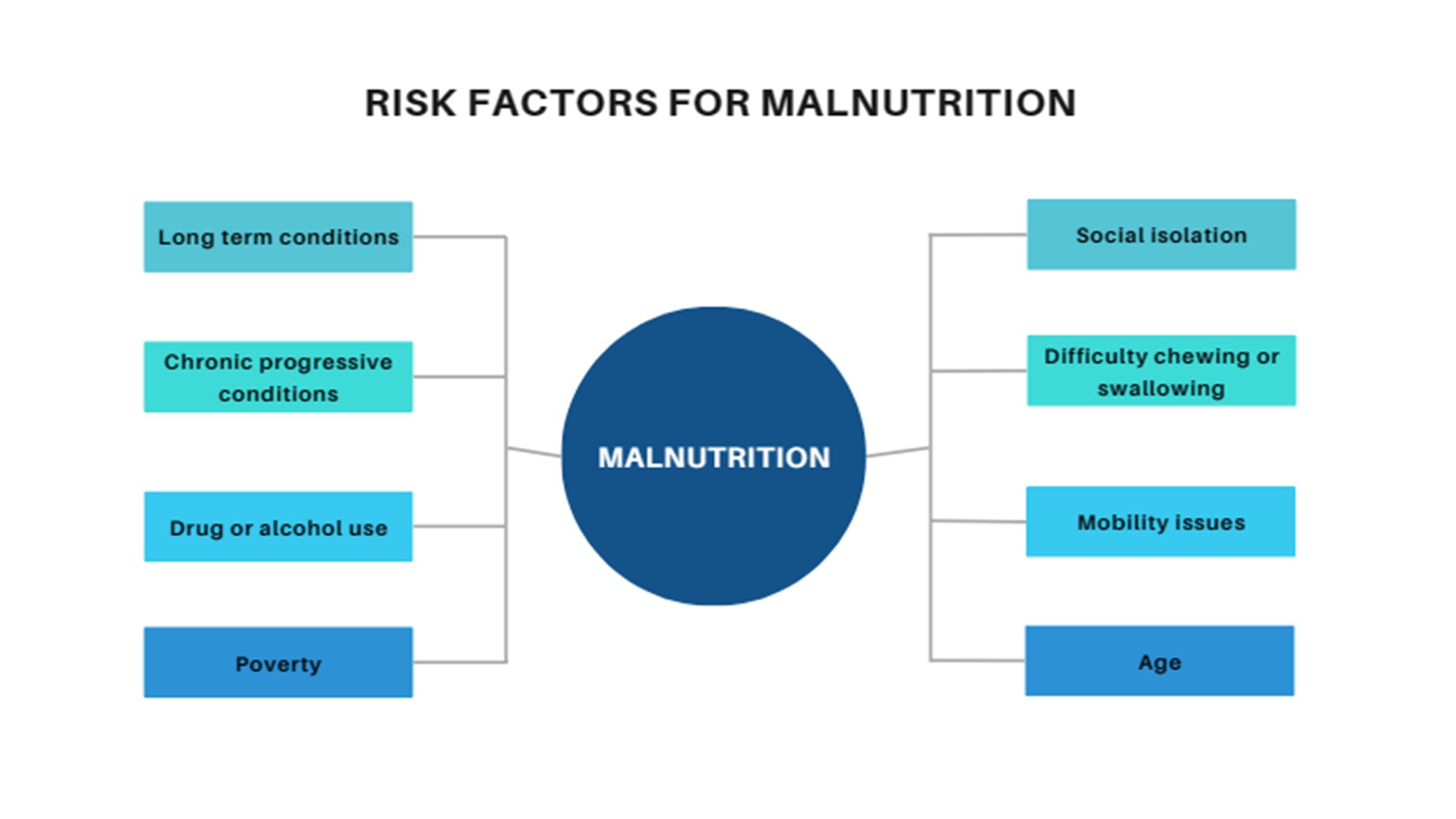
Figure 1.[10]
We are also amidst a cost-of-living crisis which is hitting many people hard. We should therefore consider that this woman may be prioritising buying cigarettes or alcohol over healthy food. She also has mobility issues, so there is a question mark over whether she can stand and cook healthy food or whether she can get out to do a food shop.
Age itself is a risk factor. She is over the age of 65, which puts her at risk of malnutrition. Other risk factors are chronic conditions such as diabetes, kidney disease, and chronic lung disease. With progressive conditions like dementia or cancer, there is also a risk of swallowing difficulties.
How does alcohol misuse contribute to malnutrition?
In small quantities alcohol is an appetite stimulant, but in larger quantities it becomes an appetite suppressant[11]. For some people it becomes a meal replacement, however, alcohol has no nutritional benefit and can interfere with absorption and storage between B12 and vitamin A[12]. The fact that the lady fell could be potentially due to night blindness from vitamin A deficiency.
Alcohol is also a diuretic[6], so it is going to increase urine output and reduce water soluble minerals such as magnesium, potassium, and zinc. Zinc can influence taste and smell[13], which might further affect dietary intake and appetite.
There are many consequences of malnutrition. It can lead to reduced ability to fight infection and impaired wound healing[14], which can lead to more GP visits, hospital admissions and prescriptions.
Malnutrition is also an independent predictor of falls in older people. Older adults who are malnourished are eight times more likely to fall than those who are well nourished[15]. In addition, if they are then admitted to hospital, 70% of patients weigh less on hospital discharge. This means that they can become stuck in a cycle of weight loss called the malnutrition carousel[16].
This can lead to muscle atrophy and can reduce a person’s ability to move around. This in turn increases the risk of falls, pressure ulcers and chest infections. Malnutrition also impacts brain function and can lead to apathy, depression, deterioration in social interactions as well as self-neglect[16] .
There are also nutritional deficiencies associated with malnutrition such as: iron deficiency; anaemia; vitamin D deficiency; and, thiamine (vitamin B1) deficiency, which can lead to Wernicke’s encephalopathy[17].
Screening for malnutrition can be carried out using the MUST screening tool – a quick and simple assessment tool which asks questions about BMI, unintentional weight loss and current appetite[18].
How would you treat malnutrition in an older patient?
There is no ‘one size fits all’ approach to treating malnutrition. In terms of our case study, we know this lady has a low BMI of 18.5 so we must examine the potential causes of unintentional weight loss and look at first line interventions such as helping with access to food, which may be home delivery for shopping or setting up a home delivery service like ‘Meals on Wheels’. I would encourage a food first approach for example having three smaller meals and three snacks throughout the day, a dessert after meals and fortify foods with butter, milk and cream[19],[20]. If their weight does not improve or deteriorates, you should refer to local nutrition pathways which may include starting a first line oral nutritional supplement and/or referring for specialist intervention from a dietitian.
Disclaimer: This webinar and webinar report was sponsored by Grünenthal Meds.
[1] UK Government Guidelines on Alcohol – https://www.gov.uk/government/publications/delivering-better-oral-health-an-evidence-based-toolkit-for-prevention/chapter-12-alcohol (accessed December 23)
[2] Royal College of psychiatrists – Our Invisible Addicts. RCP College Report CR211. March 2018. https://www.rcpsych.ac.uk/docs/default-source/improving-care/better-mh-policy/college-reports/college-report-cr211.pdf (accessed December 23)
[3] Meier P, Seitz HK. Age, alcohol metabolism and liver disease. Curr Opin Clin Nutr Metab Care 2008; 11(1): 21-6
[4] Foroughan M, Wahlund LO, Jafari Z, et al. Validity and reliability of Abbreviated Mental Test Score (AMTS) among older Iranian. Psychogeriatrics 2017; 17(6): 460-65
[5] Cristofori I, Cohen-Zimerman S, Grafman J. Executive functions. Handb Clin Neurol 2019; 163: 197-219
[6] Epstein M. Alcohol’s impact on kidney function. Alcohol Health Res World 1997; 21(1): 84-92
[7] Biddinger KJ, Emdin CA, Haas ME, et al. Association of Habitual Alcohol Intake With Risk of Cardiovascular Disease. JAMA Netw Open 2022; 5(3): e223849
[8] Caine D, Halliday GM, Kril JJ, Harper CG. Operational criteria for the classification of chronic alcoholics: identification of Wernicke’s encephalopathy. J Neurol Neurosurg Psychiatry 1997; 62(1): 51-60
[9] UK and Global Malnutrition: The New Normal. Food Foundation 2017: https://foodfoundation.org.uk/sites/default/files/2021-10/1-Briefing-Malnutrition_vF2.pdf (accessed December 2023)
[10] NHS Conditions – Malnutrition – Causes https://www.nhs.uk/conditions/malnutrition/causes/ (accessed December 2023)
[11] Healthline https://www.healthline.com/nutrition/is-alcohol-a-stimulant#depressant-effects-of-alcohol (accessed December 2023)
[12] Hoyumpa AM. Mechanisms of vitamin deficiencies in alcoholism. Alcohol Clin Exp Res 1986; 10(6): 573-81
[13] Pisano M, Hilas O. Zinc and Taste Disturbances in Older Adults: A Review of the Literature. Consult Pharm 2016; 31(5): 267-70
[14] Saunders J, Smith T. Malnutrition: causes and consequences. Clinical Medicine 2010; 10(6); 624–27
[15] Lackoff AS, Hickling D, Collins PF, et al. The association of malnutrition with falls and harm from falls in hospital inpatients: Findings from a 5-year observational study. J Clin Nurs 2020; 29: 429–36
[16] British Dietary Association The Nutrition and Hydration Digest 3rd Edition. Chapter 1: The Significance of Nutrition and Hydration. https://www.bda.uk.com/practice-and-education/nutrition-and-dietetic-practice/the-nutrition-and-hydration-digest/the-significance-of-nutrition-and-hydration.html (accessed December 2023)
[17] Thomson AD, Marshall EJ. The natural history and pathophysiology of Wernicke’s Encephalopathy and Korsakoff’s Psychosis. Alcohol Alcohol 2006; 41(2):1 51-8
[18] BAPEN. The MUST (Malnutrition Universal Screening Tool (MUST). https://www.bapen.org.uk/pdfs/must/must_full.pdf (accessed December 2023)
[19] Self Screening Tool. https://www.malnutritionselfscreening.org/ (accessed December 2023)
[20] BAPEN. Your Guide To Making the Most of Your Food – Advice for patients and carers. https://www.malnutritionselfscreening.org/pdfs/advice-sheet.pdf (accessed December 2023)

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...