Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]

Horner’s syndrome is characterised by ptosis, miosis, anhidrosis, and enophthalmos. It results from disruption of the sympathetic pathway from the hypothalamus to the eye. The aetiology in adults is dependent on the location of the lesion, which is divided into preganglionic (first- order neuron or second-order neuron lesion) and postganglionic (third-order neuron lesion).1
We present a rare case of a 60-year-old woman who presented with isolated unilateral left-sided Horner’s syndrome. Magnetic Resonance Imaging (MRI) scan of her head and neck showed a left-sided carotid body tumor. This case emphasises the need to consider carotid body tumor in patients presenting with isolated Hornor’s syndrome.
A 60-year-old woman presented to the Accident and Emergency department with a three-week history of persistent drooping of the left upper eyelid and a constricted left pupil. Neurological examination demonstrated ptosis and miosis on the left side with absent anhidrosis suggestive of a postganglionic pathology (Figure 1). The rest of the physical and neurological examination was unremarkable.

Fig 1: Unilateral ptosis and miosis on the left side
Given the isolated presentation of Horner’s syndrome, she underwent MRI of the head and neck, which revealed an ovoid-shaped well-defining lesion within the carotid bifurcation measuring 24 x 14 x 12 mm, consistent with a carotid body tumor. She was referred to Ear, Nose and Throat (ENT) surgical team.
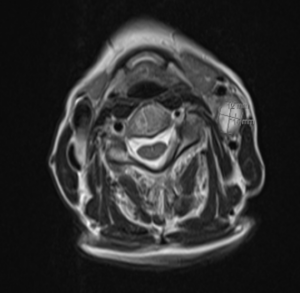
Fig 2: MRI of head and neck showing hyperintense carotid body tumour with significant splaying of the internal and external carotid arteries
Carotid body tumours (CBTs) are a common type of paraganglioma arising from the neural crest-derived carotid body.2 CBTs are rare, accounting for about 0.4% to 1.0% of arterial tumours.3 Most CBTs are benign and unilateral. They show a slightly higher incidence in women than men.4 They typically present as asymptomatic neck masses or as symptoms associated with compression of adjacent structures.5 Given the non-specific clinical presentation and complex adjacent anatomical structures, CBTs present with a higher misdiagnosis rate compared to other tumours.6
This case highlights the significance of a comprehensive diagnostic approach when investigating isolated Horner’s syndrome. Carotid body tumours should be considered in the differential diagnosis of unilateral isolated Horner’s syndrome without anhidrosis.
Pre-operative CBT diagnosis relies on imaging techniques such as Doppler ultrasound, MRI and computed tomography angiography (CTA) of the head and neck.7 Currently, treatment options offered for CBTs include surgery, radiotherapy, embolisation, or combination therapy. Surgical resection is the first line with the highest efficacy.8
Teena Thomas, SHO, East Sussex Healthcare Trust St Leonards on sea, East Sussex
Kelum Ruwanpura, Speciality Registrar, East Sussex Healthcare Trust St Leonards on sea, East Sussex
Wardah Mahmood, SHO, East Sussex Healthcare Trust St Leonards on sea, East Sussex
MJH Rahmani, Consultant Physician, East Sussex Healthcare Trust St Leonards on sea, East Sussex

This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...